
Translate this page into:
Characteristic features of neck aging

*Corresponding author: Maya Vedamurthy, RSV Skin and Research Centre, Chennai, Tamil Nadu, India. mvrsvskin@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vedamurthy M, Hande M. Characteristic features of neck aging. CosmoDerma 2022;2:35.
Abstract
In today’s era, everyone desires a youthful and beautiful look as they age. In this regard, many non-invasive and minimally invasive facial and neck rejuvenation procedures are most sought after by patients. Neck rejuvenation is of priority among patients in recent days as it significantly contributes to the overall aesthetic outcome. Therefore, as good dermatologists, we must have a sound knowledge of the anatomy of the neck, and various clinical signs of neck aging and choose the right modality of treatment with good acceptability and fewer adverse effects to obtain the desired aesthetic outcome.
Neck aging is due to intrinsic as well as extrinsic factors and manifests as skin dyspigmentation, laxity, rhytides, loss of mandibular contour, widening of the cervicomental angle, accumulation of submental fat, volume loss, and prominence of the platysmal bands. A wide range of therapeutic options is available to address these concerns. In addition, it is also imperative to advise patients to follow a good skincare regime that includes moisturizers, sunscreens, and retinol creams to have a better outcome. It is the combination approach that often produces the most optimal outcome. The treatment plan for rejuvenation must be modified for every individual based on the degree of neck aging and their expectations.
Keywords
Aging neck
Neck rejuvenation

INTRODUCTION
Youthful and attractive skin is the pursuit of many individuals. It is considered important for self-esteem and social relations.[1] There are many studies on the aging of facial skin, however, there is a paucity of literature on the age-related changes in other regions of the body.[2] In recent times, neck aging is of particular interest as patients desire a good aesthetic improvement of not only the face but also of the neck.[3] Neck aging is influenced by several factors like constant movement and sun exposure that induce skin laxity and sagging in the elderly.[4]
ANATOMY OF AGING NECK
With aging, the neck undergoes a series of changes in layers of skin, subcutaneous tissue, underlying muscles, and fascia. Hence it is imperative to understand the anatomical structures and the changes in each layer to assess the degree of aging and choose the appropriate treatment modality for rejuvenation. In addition, the anatomic transition of the neck to the lower third of the face is fundamental to the overall facial aesthetic.
Anatomically, the neck can be divided into anterior and posterior triangles. Although the posterior neck can show signs of aging, this article mainly focuses on the anterior neck. The anterior triangles of the neck are bounded inferiorly by the sternal notch and clavicles, and laterally by the sternocleidomastoid (SCM) bilaterally. The superior aspect of the anterior neck includes the chin, the lower mandibular line, and angle, rising toward the mastoid processes more posteriorly. Cartilages like the trachea, thyroid, and cricoid represent the midline, dividing right from left. Posterior to the SCM marks the start of the posterior triangle, which has trapezius, occipital scalp, and cervical vertebrae as the posterior boundaries.[5]
Skin
The skin acts as a protective barrier that is continuously in contact with the environment, undergoing not only intrinsic aging but also photoaging as a consequence of sun-induced damage from ultraviolet rays.[5] The signs of chronic photodamage and intrinsic aging are seen both on the face and neck. However, if the patient has undergone only facial rejuvenation procedures, the signs of neck aging are more obvious on the neck.[6] Clinical manifestations of the aged neck include xerosis, laxity, rhytides, and a variety of benign neoplasms like cherry angiomas, acrochordons, and seborrheic keratosis.[6] Hyperpigmentation, solar lentigines, telangiectasias, poikiloderma of Civatte, and rough texture can also be noted secondary to ultraviolet exposure.[7]
With aging, external factors, such as gravity, also play a large role in the clinical appearance of the neck. The constant force of gravity exerts a mechanical pull on the already unsupported lax skin that exposes the changes related to fat depletion, fat accumulation, or herniation, as well as the changes related to loss of structural support from the bone as the skin hangs and follows its contours.[5] Sagging is also contributed by weakened soft tissue support and diminished neuromuscular control.[6]
In histology, epidermal senescence is seen as a decrease in the number of melanocytes and Langerhans cells. Whereas, most of the histological changes occur within the dermis, which are hypocellularity, flattened dermo-epidermal junction, rete ridges and fragmented dermal collagen. This leads to fibroblast dysregulation and a decrease in the production of new collagen that clinically manifests as rhytides and lax skin.[5,7]Electron microscopy studies show loose collagen fibrers, moderate increase and thickening of elastic fibers, resorption of subepidermal fibres, decrease in the number of dermal blood vessels, and shortening of capillary loops.[6]
Subcutaneous fat
The subcutaneous fat is in between the skin and the platysma and is invested by the superficial cervical fascia. It varies in thickness according to the patient’s body habitus and weight. There can be a variable distribution of fat laterally along the surface of the platysma. It is most abundant in the submental areas, in a triangular shape with the apex at the hyoid and base at the mandibular line.[5]
With aging, there is a depletion of fat from the cervical, buccal, temporal, and perioral areas. In contrast, there is a prominent increase in the bulk of the fatty tissue in other areas like the submental areas, the nasolabial folds, and lateral malar areas. In contrast to the appearance of a young face where fat is diffusely dispersed, in aging, facial fat accumulates in pockets, and subsequently when the excess fat is subjected to the force of gravity, sagging and drooping of the skin occurs.[6]
Within the same subcutaneous plane, patients can develop prominent melolabial folds or jowls descending from the face. Although they are not neck structures, their presence has a significant impact on the perception of a youthful and aesthetically pleasing neck. These structures should be considered in the preoperative assessment, as they can be concomitantly addressed during neck rejuvenation.[5]
Superficial musculoaponeurotic system
The superficial musculoaponeurotic system (SMAS) is a continuous, organized fibrous network within the face, contiguous with platysma as it extends from the face into the neck. The SMAS is a multidimensional structure consisting of collagen and elastic fibers, fat cells, and muscle fibers. These fibrous extensions have a course from the periosteum or musculature through the subcutaneous layers connecting with the dermis allowing movement of all the layers as a single unit.[8]
Platysma
The platysma is a muscle situated between the superficial and deep cervical fascia and separates the subcutaneous fat from the deeper structures of the neck. The platysma takes its origin from the superficial fascia overlying the superior aspect of the deltoid and pectoralis major and inserts to the mandible, depressor anguli oris, risorius, and mentalis superiorly. The platysma is contiguous with the SMAS in the face with innervated by the cervical branch of the facial nerve.
With aging, the platysma begins to lose tone and is pulled laterally, resulting in splaying of the medial fibers. Also, there is attenuation of the deeper ligaments on the medial edge of the muscle contributing to a loss of tone, leading to the development of platysmal bands. Patients with minimal or no platysmal decussation can also have interplatysmal fat in the submental region herniate between the medial edges, further contributing to the clinical appearance of an aging neck.[5]
Bone
Mandible
The aesthetic appearance and impression of youth can be greatly influenced by the superficial topography of the mandible. The facial skeleton undergoes resorption showing reduced mass with age. It particularly affects the mandible, maxilla, and frontal bones. Bone loss in these areas enhances the facial droopiness and contributes to the obliterated demarcation between the contour of the jaw and neck.[6] Other factors like jowling, fat descent, and submental fullness also influence changes in mandibular contour resulting in loss of mandibular definition.[5]
Hyoid
The hyoid and its relationship to the muscular, bony, and fascial attachments take on a vital role in establishing the CMA. The hyoid bone typically lies at the level of the third cervical vertebrae and this position relative to the mandible corresponds with the cervicomental angle (CMA). A low anterior hyoid results in the appearance of an obtuse CMA.[5]
Pathogenesis
Aging is an inevitable universal phenomenon. It is affected by a genetic program along with cumulative environmental and endogenous insults. Skin aging can be intrinsic as well as due to extrinsic factors such as visible, ultraviolet, and infrared rays in the sunlight, smoking, and air pollution. Both result in the formation of reactive oxygen species during oxidative cellular metabolism causing cumulative endogenous damage to cellular constituents. Other factors include shortening of chromosomal telomeres, hormonal influences, as well as age-associated, a decline in anabolic signaling molecules, and upregulation of the reciprocal catabolic factors.[5,7] These cellular events result in progressive degradation of collagen and elastin that clinically translates as xerosis, laxity, and wrinkles.[2,7] Changes in the platysma and local subcutaneous fat accumulation are also associated with age-related changes in the neck area. Also, a constant movement of the neck influences the formation and aggravation of wrinkles in the neck.[2] The constant force of gravity also contributes to a great extent to the aging neck as it exerts a mechanical pull on the already unsupported and lax skin.[7] The factors responsible for neck aging have been summarized in Figure 1.
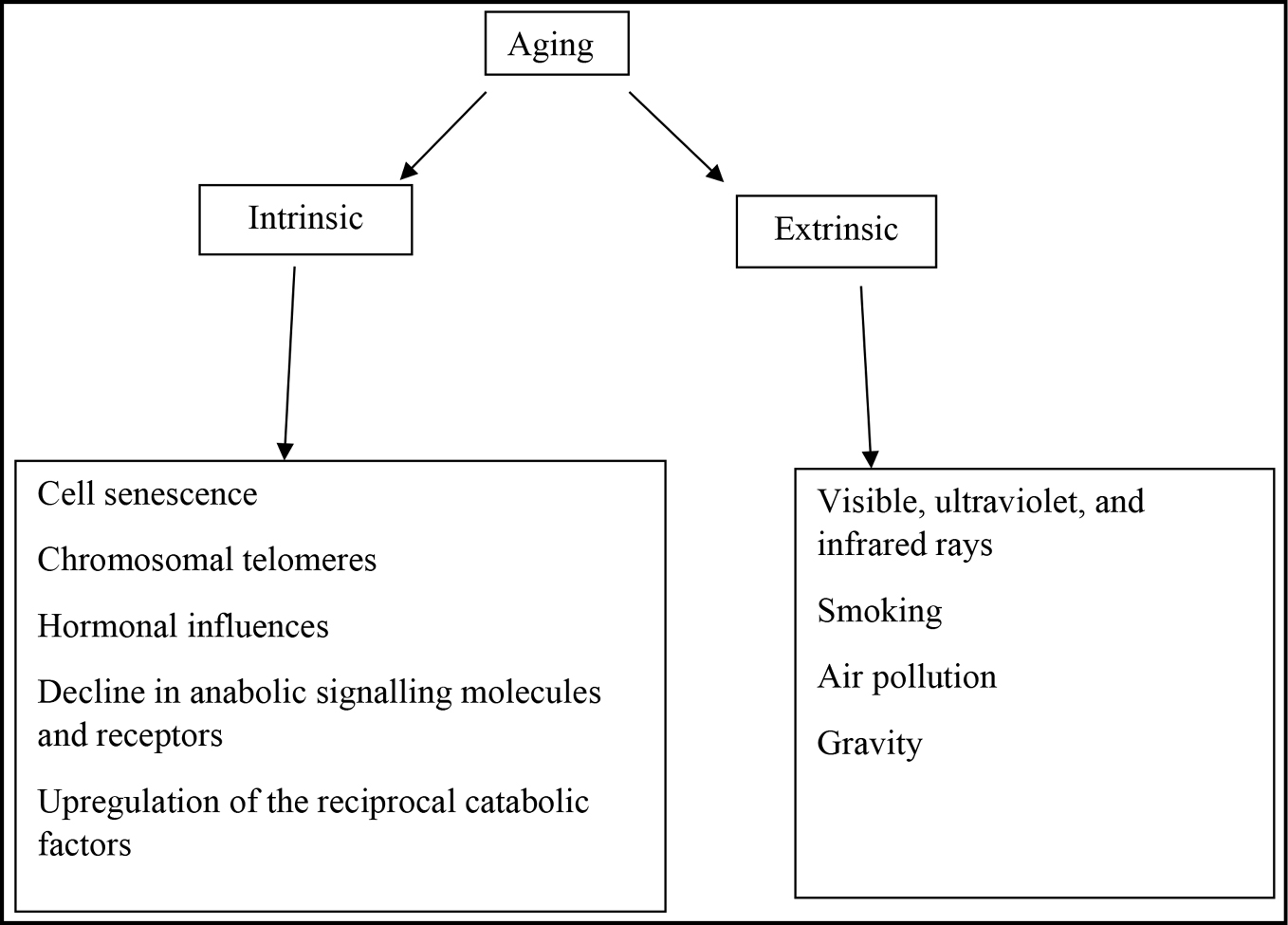
- Factors influencing neck aging.
Clinical features
Neck aging manifests with various clinical characteristics like horizontal neck rhytides, sagging, hollowing of the emaciated neck, prominence of platysmal bands, and alteration in skin texture.[2] The aesthetic neck classification helps the dermatologist to evaluate the severity of aging and to plan the treatment accordingly [Table 1].
| Category | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Skin | Normal | Mild to moderate laxity | Mild to moderate laxity | Mild to moderate laxity | Normal or mild to moderate laxity | Laxity in the neck only | Laxity in neck cheek and jowls |
| Fat | Any excess | Normal | Mild to excessive | Moderate to severe | Normal or any fat excess | Normal or any fat excess | Normal or any fat excess |
| Muscle | Normal | Normal | Normal | Normal | Slight upper banding | Moderate to full platysmal bands | Moderate to full platysmal bands |
Treatment
In comparison to facial rejuvenation, the neck is much neglected. Sunscreen with a broad spectrum of action, moisturizers, and topical retinoid-based skincare products must be incorporated into daily skincare regimes to delay the clinical signs of neck aging. Frequent and prolonged baths, use of detergent soaps and foams should be avoided which could lead to dryness of the skin.[9]
Treatment of aging neck has a wide variety of surgical and non-surgical options. Good candidates for neck rejuvenation are patients who have moderately thick skin, minimal sun damage and who have retained some hereditary elasticity appropriate for their chronological age.[5]
With the increasing demand for minimally invasive cosmetic procedures, various non-invasive devices have been developed for skin tightening and lifting the skin over the neck. The commonly used nonsurgical neck contouring modalities include radiofrequency, light-based devices, ultrasound devices, thread lifting, botulinum toxin, and fillers [Tables 2 and 3]. Grade 1–5 of aesthetic neck classification can be satisfactorily managed with non-surgical options. It is only in grades 6 and 7 with moderate to the full platysma, surgical interventions may be sorted.
| Procedure | Mechanism of action | Targeted tissue |
|---|---|---|
| Radiofrequency | High-frequency radio waves | Dermis and subcutaneous tissue |
| High-intensity focused ultrasound | Ultrasonic waves | Dermis and subcutaneous tissues down up to platysma |
| Light-based devices- a. IPL b. Ablative c. Fractional | Pigmented lesions, target chromophore-melanin Target chromophore-water | Epidermis and dermis Epidermis and dermis Dermis |
| Thread lifting | Mechanotransduction | Dermis and subcutaneous Tissue |
| Botulinum toxin | Chemical denervation | Muscle |
| Fillers | Mechanical filling and Neocollagenesis | Subdermis |
| Cryolipolysis | Controlled cooling of adipocytes | Subcutaneous tissue |
| Lipolytic injections | Lipolysis | Subcutaneous tissue |
| Signs of neck aging | Treatment modalities |
|---|---|
| Dyspigmentation | Intense pulsed light (IPL) |
| Laxity | Radiofrequency devices High-intensity focused ultrasound Fractional lasers Thread lifting |
| Alteration of skin texture | Fractional lasers Threads |
| Rhytides | Fillers Threads |
| Loss of mandibular contour | Fillers Threads |
| Submental fat accumulation | Cryolipolysis Lipolytic injections |
| Volume loss | Fillers |
| Prominent platysmal bands and horizontal neck bands | Botulinum toxin |
Radiofrequency devices
Radiofrequency (RF) functions via the emission of electromagnetic current of high frequency that generates heat in the dermis and subcutaneous tissues. Heating the dermal tissue to 42°C allows for immediate tightening of the collagen triple helix via breakdown of hydrogen bonds in the collagen, causing shrinkage of the normal collagen structure, as well as induction of the healing cascade, leading to neocollagenesis, elastin remodeling, and angiogenesis over the following 3–4 months.[10]
High-intensity focused ultrasound
High-intensity focused ultrasound (HIFU) delivers inducible ultrasonic energy to discrete areas while preserving the superficial skin and producing clinically satisfactory results independent of Fitzpatrick skin types. Hence it is one of the commonly preferred non-surgical procedures for neck rejuvenation. Following HIFU, collagen and elastic fibers are significantly increased in the deep reticular dermis contributing to the deep tissue tightening.[3] The most common adverse effect reported was pain during the procedure followed by erythema and swelling which were mild and transient.[3]
Micro focused ultrasound with visualization (MFU-V)
Micro-focused ultrasound with visualization (MFU-V) is a safe non-invasive method to address mild to moderate laxity in the jowl or neck area. It delivers highly focused ultrasound energy to precise subdermal targets without disrupting surrounding tissues resulting in immediate contraction of denatured collagen, neocollagenesis, and collagen remodeling.[6]
Light-based devices
Intense pulsed light (IPL) is very effective in treating dyspigmentation, telangiectasia, and poikiloderma of Civatte, with minimal adverse events. The use of IPL on the neck not only results in clearance of more than 75% of hyperpigmentation and telangiectasia but can also improve texture.[7]
Ablative lasers such as CO2 and Erbium remove the upper layer of the skin, allowing for natural epidermal and dermal regeneration for a new, better-looking skin. These devices are effective resurfacing options, but are usually painful and involve considerable recovery time with possible infectious and pigmentation risks.[12]
In recent years, the concept of fractional photothermolysis has become very popular. The fractional CO2 laser produces an array of microthermal treatment zones in a pixelated fashion, with a confluent pattern of ablation and coagulation. It extends from the stratum corneum through the dermis. Rapid wound healing is due to the viable keratinocytes present in the untreated islands of the surrounding skin. A fractional laser is therefore safe and effective for skin tightening and texture improvement.[13]
Thread lifting
Threads can be used to improve skin texture, wrinkling, and laxity to achieve an ideal aesthetic appeal. They allow the skin of the neck and face to be in sync, with minimal discomfort or downtime. Threads work by providing a continuous mechanical stimulus to the cell, a process known as mechanotransduction. It increases cellular metabolism and induces the production of new collagen.[14] Polydioxanone (PDO) and poly l-lactic acid (PLLA) threads are commonly used. It stimulates fibroblast, collagenization, and neo-angiogenesis. The common side effects are mild bruising and edema.[15]
Botulinum toxin
Botulinum toxin is one of the age-old procedures for the face and neck rejuvenation. By chemical denervation, they relax the medial platysma bands. This results in enhanced acuity of the cervicomental angle and reduced visibility of the aging appearance of the medial cords.[12] Careful selection for patients who have obvious platysmal bands, good cervical skin elasticity, and minimal fat descent is necessary for a good outcome.
Horizontal necklace lines of skin indentation are noted in a slightly chubbier neck caused by the superficial musculoaponeurotic system attachments. Aliquots of 1 to 2U are injected in the deep intradermal plane at 1-cm intervals along the horizontal necklines to soften them. Up to 15–20U of botulinum toxin can be injected for horizontal lines per treatment session.[17] Other indications include lateral platysmal bands, poorly defined jawlines, necklace lines, prominent digastric muscles, and prominent submandibular glands.[12] Cervical dysphasia, swallowing difficulty, asymmetry, and sternocleidomastoid weakness are the reported rare side effects.[17]
Fillers
For patients who have fine rhytides and horizontal lines, subdermal injections of particulate biostimulants such as polylactic acid can result in stimulation and a neo-collagenesis, with thickening of the dermis. Injections of hyaluronic acid gel in the subdermal space or protein-rich plasma have also been used for neck rejuvenation. Most often, adverse effects are transient. They include injection site-related reactions of mild intensity, including erythema, pruritus, ecchymosis, and localized swelling.[18]
Cryolipolysis
Cryolipolysis is a popular technique that produces non-invasive fat reduction by controlled cooling of adipocytes that is widely used to treat various locations on the body including submental fat. As with treatment elsewhere in the body, cryolipolysis of submental fat may require multiple sessions to achieve the desired effect.[7]
Lipolytic injections
The administration approved deoxycholic acid injection, which when injected locally promotes lipolysis resulting in the reduction of fat bulk. Improvement is often noted at 12 weeks follow-up after a series of four injections spaced approximately one month apart.[7]
CONCLUSION
Although there are wide therapeutic options available for the prevention and treatment of neck aging, they have to be tailored to individual patients’ expectations and the severity of aging. Sound knowledge of anatomy, and choosing the suitable modality of rejuvenation are important for a good aesthetic outcome. A combination approach with a good daily skincare regime including moisturizers, sunscreen, and retinol creams along with non-invasive energy-based devices gives a good outcome. Different modalities of treatment can also be combined to result in faster and desired improvement.
Declaration of patient consent
Patient consent is not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Evaluation of skin aging: A systematic review of clinical scales. Br J Dermatol. 2015;172:1249-61.
- [CrossRef] [PubMed] [Google Scholar]
- Characteristic features of neck skin aging in Chinese women. J Cosmet Dermatol. 2018;17:935-44.
- [CrossRef] [PubMed] [Google Scholar]
- Synergistic effect of high-intensity focused ultrasound and low-fluence Q-switched Nd:YAG laser in the treatment of the aging neck and décolletage. Lasers Med Sci. 2017;32:109-16.
- [CrossRef] [PubMed] [Google Scholar]
- Age-related changes in skin bio-mechanical properties: The neck skin compared with the cheek and forearm skin in Korean females. Skin Res Technol. 2013;19:236-41.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomy and physiology of the aging neck. Facial Plast Surg Clin North Am. 2014;22:161-70.
- [CrossRef] [PubMed] [Google Scholar]
- Neck rejuvenation using a combination approach: Our experience and a review of the literature. Dermatol Surg. 2016;42:S94-S100.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and histological features of intrinsic versus extrinsic skin aging. 2006
- [CrossRef] [Google Scholar]
- Anatomy of the SMAS revisited. Aesthetic Plast Surg. 2003;27:258-64.
- [CrossRef] [PubMed] [Google Scholar]
- Antiaging therapies. Indian J Dermatol Venereol Leprol. 2006;72:183-186.
- [CrossRef] [PubMed] [Google Scholar]
- Radiofrequency for the treatment of skin laxity: Mith or truth. An Bras Dermatol. 2015;90:707-21.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A novel noninvasive radiofrequency dermal heating device forskin tightening of the face and neck. J Cosmet Laser Ther. ;17:307-12.
- [CrossRef] [PubMed] [Google Scholar]
- Neck rejuvenation with fractional CO2 laser: Long-term results. J Clin Aesthet Dermatol. 2014;7:23-9.
- [PubMed] [PubMed Central] [Google Scholar]
- The nonsurgical thread lift for facial rejuvenation. Nonsurgical lip and eye rejuvenation techniques 2016:85-95.
- [CrossRef] [Google Scholar]
- Neck rejuvenation with thread lift. J Cutan Aesthet Surg. 2019;12:196-200.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Nonexcisional, minimally-invasive rejuvenation of the neck. Clin Plastic Surg. 2014;41:11-31.
- [CrossRef] [PubMed] [Google Scholar]
- Aesthetic botulinum A toxin in the mid and lower face and neck. Dermatol Surg. 2003;29:468-76.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of horizontal neck wrinkles with hyaluronic acid filler: A retrospective case series. Plast Reconstr Surg Glob Open. 2019;7:e2366.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




