
Translate this page into:
Penile granuloma annulare: An uncommon entity

*Corresponding author: Jayati Shailesh Dave, Department of Dermatology, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India. jayatidave20@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh S, Dave JS, Mahajan SA, Kharkar V, Maheshwari A, Kamble PD. Penile granuloma annulare: An uncommon entity. CosmoDerma 2023;3:107.
Abstract
Granuloma annulare (GA) is a benign inflammatory disorder of unknown etiology, histologically characterized by dermal palisading granulomas with central degeneration of collagen. Involvement of the penis is exceptional and lesions restricted only to the glans penis are rarely reported. We report a middle-aged male, presenting with asymptomatic plaques on the glans penis which on biopsy proved to be interstitial GAs. Penile GA seldom shows spontaneous resolution as in our case. Penile GA although rare should be considered in the differential diagnosis of granulomatous lesions of the penis and histological examination is crucial for its diagnosis to avoid over-treatment.
Keywords
Penile
Granuloma annulare
Histopathology

INTRODUCTION
Granuloma annulare (GA) is an uncommon benign, granulomatous inflammatory cutaneous lesion that has no proven etiology and is often self-resolving. It usually involves the hands and feet, commonly in young females.[1-3] It is associated with diabetes mellitus, thyroid disease, mild trauma, hyperlipidemia, infections (Epstein–Barr virus, human immunodeficiency virus, varicella-zoster virus, and tuberculosis), vaccines, malignancy, and certain drugs (tumor necrosis factor [TNF]-alpha inhibitors).[4] Very few cases of penile GA have been reported.
CASE REPORT
A 50-year-old healthy male presented with asymptomatic raised lesions over the glans for 1 year. There were no other genitourinary complaints or any history suggestive of high-risk sexual behavior. On examination, there were multiple skin-colored firm and smooth papules which were coalescing to form plaques over the glans penis [Figures 1 and 2]. The papules were non-tender and the overlying skin was intact. There was no inguinal or femoral lymphadenopathy. Our differential diagnosis was genital warts, lichen planus, GA, and sarcoidosis. Routine hematological and biochemical tests were normal. Human immunodeficiency virus, hepatitis B, hepatitis C, syphilis serology including Venereal Disease Research Laboratory, and treponema pallidum hemagglutination were negative. Angiotensin-converting enzyme levels were normal.
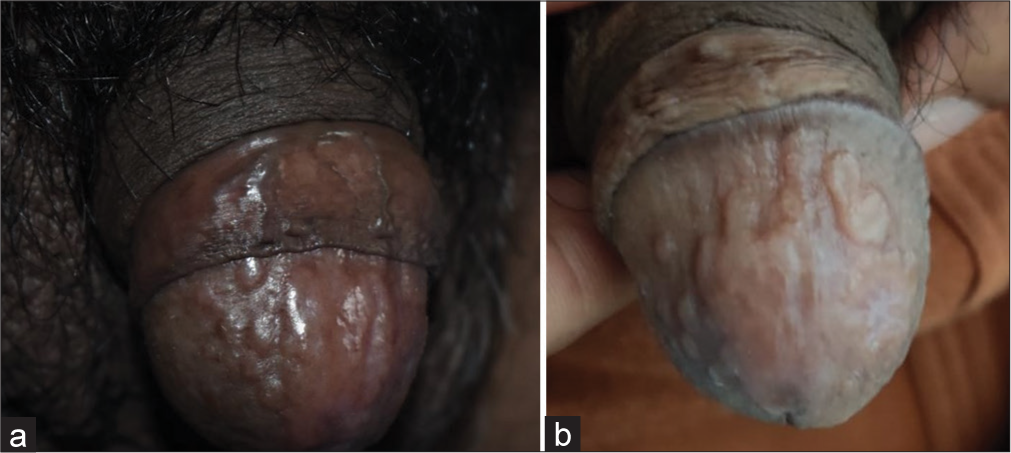
- (a and b) Clinical image showing multiple skin-colored papules coalescing to form plaque.
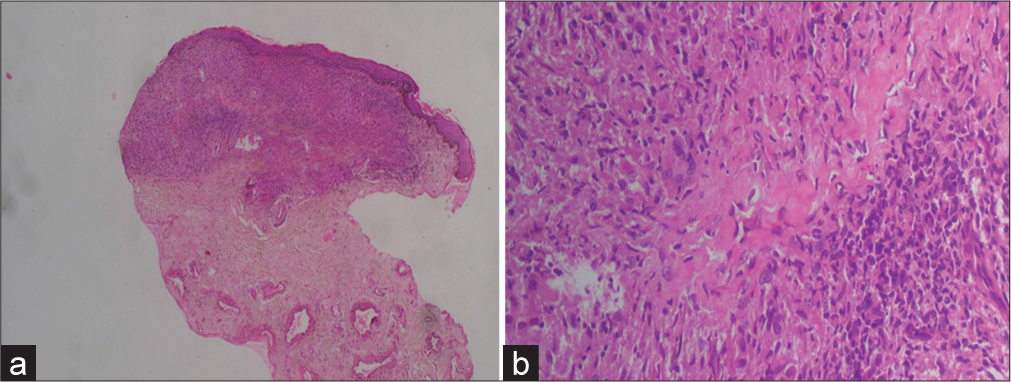
- (a) The histopathology section showing granulomatous changes around degenerated collagen (Hematoxylin and Eosin stain ×10). (b) The histopathology section showing necrobiotic collagen with palisade of histiocyte surrounding it (Hematoxylin and Eosin stain ×40).
A biopsy from the papule, under scanner showed a granulomatous reaction involving the whole of the dermis. On higher magnification, there was interstitial infiltrate of histiocytes with a central core of necrobiotic collagen [Figures 2a and b] consistent with interstitial GA. The patient was treated with mometasone 0.05% cream bd for 15 days and was switched to tacrolimus 0.03% ointment with little improvement, and there was persistent induration. Pentoxifylline 400 mg thrice daily was added for 1 month which showed a marked response in the form of a decrease in the induration of the lesion.

- Post-treatment clinical image showing the resolution of papules and plaques over the glans.
DISCUSSION
GA is a necrobiotic disorder of unknown etiology. It is often seen over acral sites such as the dorsum of hands, elbows, and feet and involvement of the penis is rare.[5-8] There are different types of GA, they are – annular (localized), generalized (disseminated), nodular (subcutaneous), and perforating forms. Histopathology of GA shows a palisade of histiocytes around a focus of necrobiosis, increased mucin deposition, and multinucleated giant cells. Clinically, the differential diagnosis includes sexually transmitted diseases, benign neoplasms, annular lichen planus, and psoriasis. Very few cases of penile GA have been reported and lesions restricted to the glans penis are even less. Treatment modalities include surgical excision, intralesional corticosteroids,[9] topical tacrolimus, carbon-dioxide laser treatment,[10] low-dose intralesional injections of recombinant human interferon-gamma,[11] and pentoxifylline. The mechanism of action of pentoxifylline in GA is not known, but it is postulated that it has TNF-alpha blocking action, inhibition of macrophage activation, and hence granulomatous inflammation. It also reduces the blood viscosity and hence increases oxygenation.[12] Penile GA seldom shows spontaneous resolution, unlike other forms.[9]
CONCLUSION
Penile GA although rare should be considered in the differential diagnosis of granulomatous lesions of the penis and histological examination is crucial for its diagnosis to avoid over-treatment. We report this case for an uncommon presentation of GA at an unusual site.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- The interstitial variant of granuloma annulare: Clinicopathologic study of 69 cases with a comparison with conventional granuloma annulare. J Cutan Pathol. 2019;46:471-8.
- [CrossRef] [PubMed] [Google Scholar]
- Lack of an association between generalized granuloma annulare and malignancy: A case-control study. J Am Acad Dermatol. 2019;80:1799-800.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatoscopy of granulomatous disorders. Dermatol Clin. 2018;36:369-75.
- [CrossRef] [PubMed] [Google Scholar]
- Penile granuloma annulare of an adolescent male-case report and review of the literature. Pediatr Dermatol. 2008;25:260-2.
- [CrossRef] [PubMed] [Google Scholar]
- Palisading granuloma of the penis: A variant of subcutaneous granuloma annulare. Ann Dermatol Venereol. 2002;129:1046-8.
- [Google Scholar]
- Granuloma annulare localized to the shaft of the penis. Scand J Urol Nephrol. 1993;27:549-51.
- [CrossRef] [PubMed] [Google Scholar]
- CO2 laser and granuloma annulare. J Dermatol Surg Oncol. 1988;14:120.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of granuloma annulare by local injections with low-dose recombinant human interferon gamma. J Am Acad Dermatol. 1998;39:117-9.
- [CrossRef] [PubMed] [Google Scholar]
- Generalised granuloma annulare successfully treated with pentoxifylline. Australas J Dermatol. 1993;34:103-8.
- [CrossRef] [PubMed] [Google Scholar]




