
Translate this page into:
Eruptive syringomas – An uncommon presentation in a male

-
Received: ,
Accepted: ,
How to cite this article: Dhawan S, Gakhar A, Sharma K. Eruptive syringomas – An uncommon presentation in a male. CosmoDerma 2023;3:100.
Abstract
Syringomas are benign adnexal tumors derived from the intraepidermal portion of eccrine glands. They are mostly found in young to middle aged women as asymptomatic (sometimes pruritic), soft, and yellowish-brown or skin-colored papules with bilaterally symmetrical distribution. The lesions have a predilection for periorbital area (primarily lower eyelids) and cheeks. A variant-eruptive syringoma presents as successive crops of disseminated lesions in atypical areas. There are very few reports of such cases. Therefore, we report this rare variant of syringoma in a male on an unusual site.
Keywords
Syringomas
Eruptive
Male

INTRODUCTION
The word syringoma is derived from a Greek word syrinx meaning a pipe or a tube[1] Syringoma is a benign, adnexal tumor derived from intraepidermal eccrine ducts.[2] It is mostly found in the periorbital skin of young- and middle-aged women.[3] Clinically, the lesions appear as multiple, small (1–3 mm in diameter), mostly asymptomatic (sometimes pruritic), and yellowish-brown or skin-colored papules.[4] Friedman and Butler proposed a clinical classification for syringomas: A localized form, generalized form (multiple and eruptive), familial form, and a form associated with Down’s syndrome.[5] Eruptive syringoma is a rare variant first described by Jacquet and Darier in 1887. Eruptive syringomas have non-specific presentation and findings. The lesions occur in successive crops on atypical sites such as anterior chest, neck, abdomen, and axillae.[6] Sometimes the lesions can be associated with mild itch. The lesions are benign and can sometimes spontaneously resolve or remain stable. The treatment remains cosmetic but relapses are frequent.[7]
Eruptive syringomas on such atypical sites in a male are a rare condition with very few reported cases in the literature.
CASE REPORT
A healthy 22-year-old male presented to our OPD with asymptomatic, persistent, and hyperpigmented papules on anterior neck since 7 years. These lesions started appearing during puberty on the neck. In the months following the initial presentation, there was a sudden increase in the size and number of these papules, spreading to the entire neck, chest, and face. No other body part was involved. No family history of similar lesions was present.
On examination, there were 30–40 red to brown colored, well-defined papules which were 2–5 mm in size, and scattered over entire neck and chest. On close examination, very few small lesions could be appreciated around eyes as well [Figures 1 and 2].

- A 27-year-old male patient presenting with multiple hyperpigmented, asymptomatic papules measuring 2–5 mm in size, scattered on the upper part of the chest and neck chest in a bilaterally symmetrical distribution.
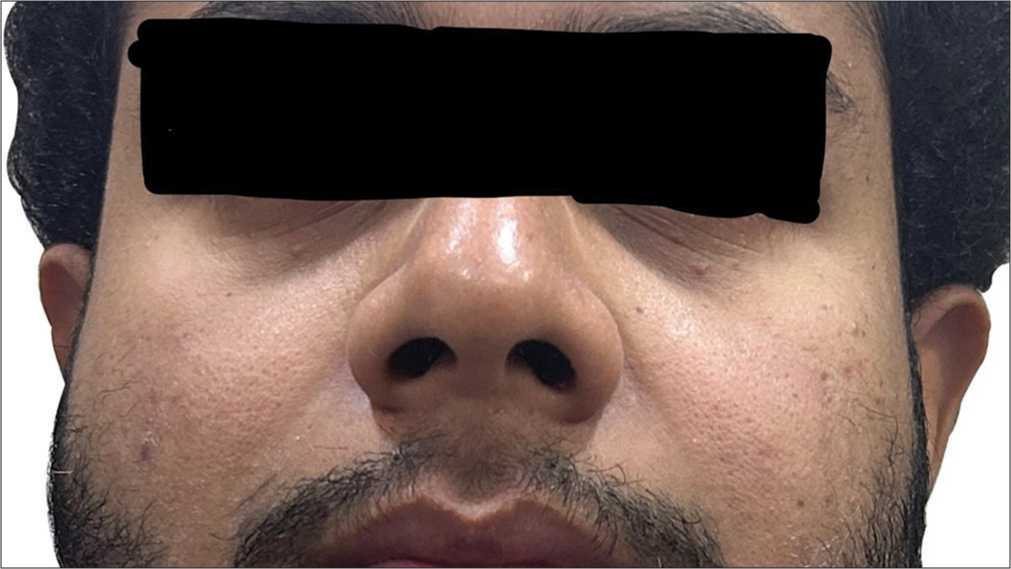
- Presence of few papules papules on the face, around eyes.
A single 4 mm punch biopsy of an entire papule on left side of the neck was taken. The histopathology report on magnification ×2 and ×10 revealed epithelial cells forming ductules, nests, and cysts in a sclerotic stroma with eosinophilic debris. The patient’s clinical picture coupled with the histopathologic findings was consistent with the lesions being syringomas [Figure 3].
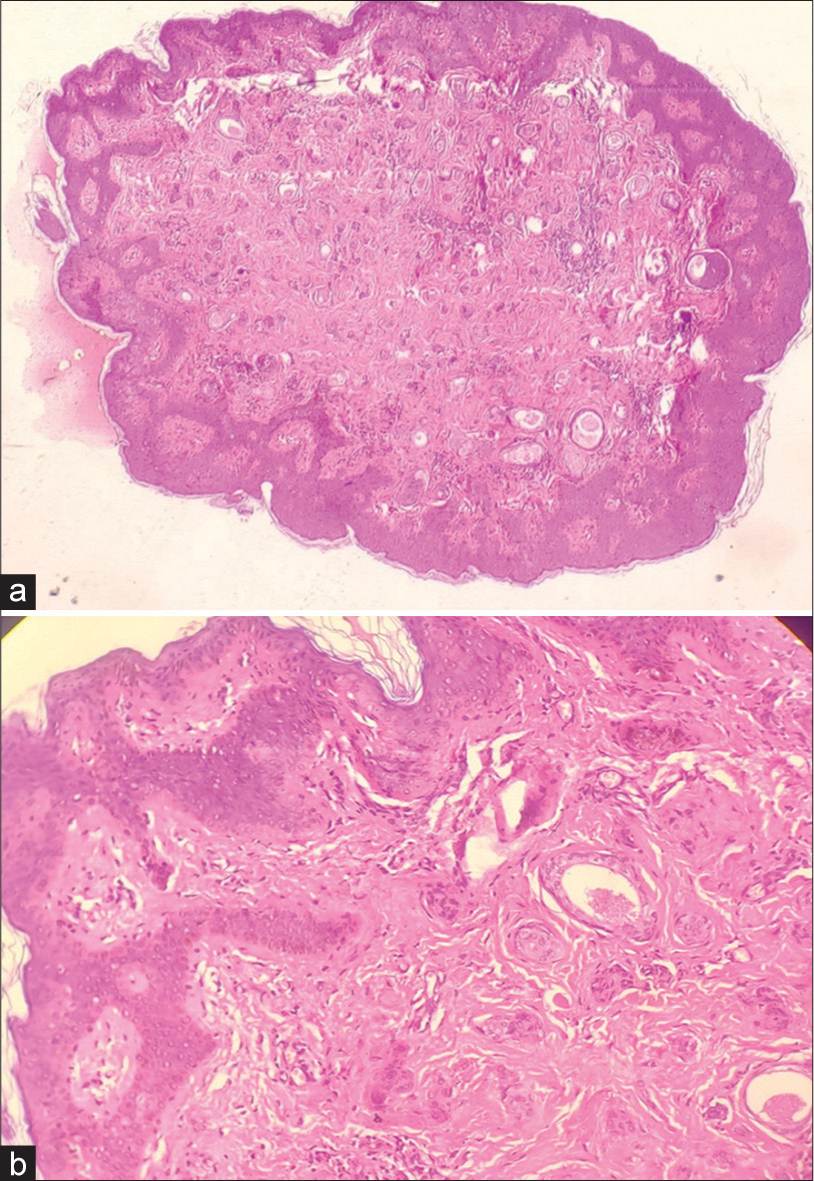
- Hematoxylin and Eosin stained section (aX40 magnification, b-X100 magnification) showing multiple ducts and cysts lined by epithelial cells, presents in a sclerotic stroma with eosinophilic debris.
DISCUSSION
Syringomas were initially described by Kaposi as benign adnexal tumors of eccrine sweat duct.[8] The lesions appear as 1–3 mm, yellowish-brown or skin-colored papules distributed in symmetrical pattern.[4] There have been reports of unilateral, nevoid, bathing trunk, and generalized distribution of syringoma.[9] Although commonly found at the time of puberty or in middle aged women in the periorbital skin, eruptive syringomas appear as numerous disseminated papules appearing in successive crops on anterior aspect of neck, chest, trunk, axilla, arms, or genitalia.[8,10] Estrogen and progesterone receptors have been detected in histochemical studies of syringomas, explaining the increased incidence of syringomas in females during puberty.[11] This makes occurrence of syringomas in males an uncommon and rare presentation.
Eruptive syringoma is a very rare variant with non-specific clinical findings, making clinical diagnosis tough. Due to variable presentation and due to similarity with other diseases such as acne vulgaris, sebaceous hyperplasia, lichen planus, warts, eruptive vellus hair cysts, papular mucinosis, steatocystoma multiplex, and mastocytosis, the final diagnosis is made on the basis of histological examination.[1,12] The histopathology shows that epidermis is unremarkable. Dermis shows multiple ducts and small solid epithelial nests, cords or tubules embedded in a sclerotic stroma. These ducts are lined by rows of epithelial cells with pale, eosinophilic cytoplasm, and rounded monomorphic nucleus. Some ducts possess small, comma-like tails of epithelial cells. This gives the duct a tadpole like appearance.[13] A study by Ghanadan and Khosravi presented some case with acanthosis, hyperpigmentation of basal keratinocytes, milia-like cysts, and telangiectasia of superficial vessels.[2]
Eruptive syringomas have no long-term associated morbidity or mortality.[14] Therefore, the treatment of syringomas is only for cosmesis. Various treatment options are available, but the main idea of treatment is to prevent scarring and recurrence. Surgical excision, electrocoagulation, ablative carbon dioxide laser, dermabrasion, and liquid nitrogen cryotherapy yield poor cosmetic results.[3] Oral isotretinoin, topical tretinoin, and adapalene have shown partial improvement in very few case reports.[14,15,16] Although the treatment options are abundant, the results are unsatisfactory. Surgical modalities may cause scarring and post inflammatory hyperpigmentation and none of them prevent recurrences. This makes treatment of syringomas frustrating.
CONCLUSION
Although eruptive syringoma is not an uncommon variant, these eruptions have a female preponderance that too, commonly on face. The presence of eruptive syringoma in a male, that too, in an unusual site of chest and neck, makes this a rare case worth reporting.
This case report is also an indication that while examining a case of syringoma, dermatologists should examine the extrafacial sites as well.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Eruptive syringoma-a great mimicker: An uncommon presentation in males. Int J Health Allied Sci. 2014;3:270-2.
- [CrossRef] [Google Scholar]
- Cutaneous syringoma: A clinicopathologic study of 34 new cases and review of the literature. Indian J Dermatol. 2013;58:326.
- [CrossRef] [PubMed] [Google Scholar]
- Generalized eruptive syringomas. Indian J Dermatol. 2009;54:65-7.
- [CrossRef] [PubMed] [Google Scholar]
- Syringoma: A review of twenty-nine cases. Acta Derm Venereol. 1998;78:460-2.
- [CrossRef] [PubMed] [Google Scholar]
- Syringoma presenting as milia. J Am Acad Dermatol. 1987;16:310-4.
- [CrossRef] [PubMed] [Google Scholar]
- Eruptive hydradenomas, adenoid epitheliomas of the sweat glands or sweat adenomas. Ann Dermatol Syph. 1887;8:317-23.
- [Google Scholar]
- Appendage tumors and hamartomas of the skin In: Goldsmith L, Katz S, Gilchrest B, Paller A, Leffell D, Wolff K, eds. Fitzpatrick's Dermatology in General Medicine (8thed). USA: McGraw Hill; 2012. p. :1348-9.
- [Google Scholar]
- Familial eruptive syringomas: Case report and review of the literature. J Cutan Med Surg. 2013;17:84-8.
- [CrossRef] [PubMed] [Google Scholar]
- Progesterone receptor positivity supports hormonal control of syringomas. J Cutan Pathol. 1995;22:442-5.
- [CrossRef] [PubMed] [Google Scholar]
- Late-onset of eruptive syringomas: A diagnostic challenge. An Bras Dermatol. 2015;90(3 Suppl 1):239-41.
- [CrossRef] [PubMed] [Google Scholar]
- Eruptive hidradenoma and syringoma. Histological, histochemical, and electron microscopic studies. Arch Dermatol. 1967;96:500-19.
- [CrossRef] [PubMed] [Google Scholar]
- An unusual case of generalised eruptive syringoma in an adult male. Med J Armed Forces India. 2014;70:389-91.
- [CrossRef] [PubMed] [Google Scholar]




