
Translate this page into:
Skincare in the elderly: An ignored domain

*Corresponding author: Priyansh Gupta, Department of Dermatology, Venereology and Leprosy, AIIMS, Bhubaneswar, Odisha, India. priyansh.gupta2412@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sangwan P, Gupta P. Skincare in the elderly: An ignored domain. CosmoDerma 2023;3:138.
INTRODUCTION
Elderly skin differs from that of younger individuals in being as fragile and reactive as of newborns, thus requiring special care. The multitude of skin changes occurs with age and the factors responsible are represented in Figure 1.[1,2] Likewise, many age-related changes are seen in other skin appendages such as hairs and nails which have been discussed in subsequent sections. All this requires special attention and proper care so that elderly people are able to adore the beauty of their skin.
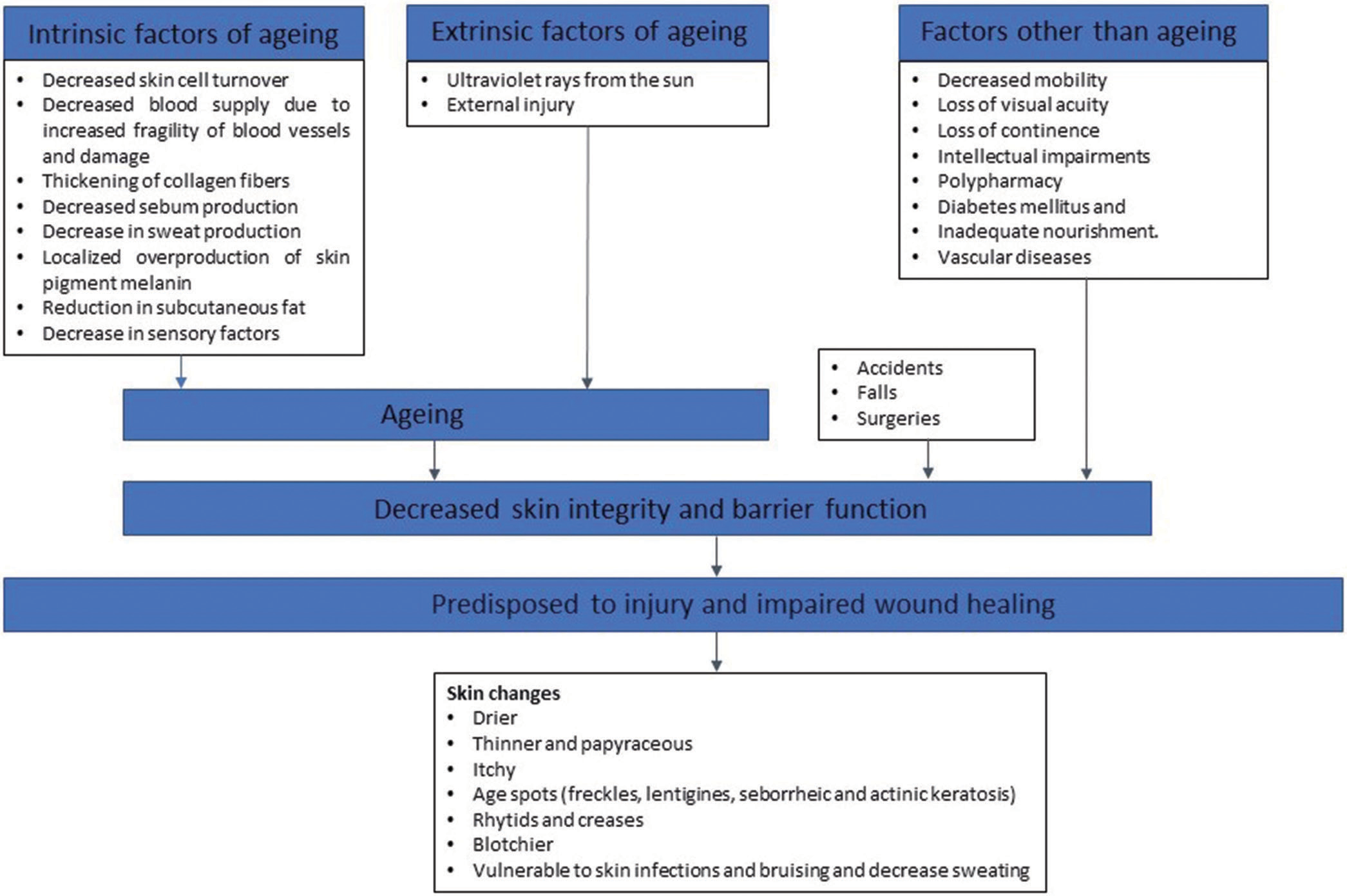
- Flowchart showing the various intrinsic and extrinsic factors leading to aging of the skin and other factors which lead to skin damage and decrease barrier function of the skin.
SKIN
Majority of elderly individuals suffer from skin problems, the most common being itch (senile-itch) and xerosis, both of which can be idiopathic or secondary to primary cutaneous diseases/systemic ailments.[1] Psychogenic or Willan’s itch is a well-recognized idiopathic form without primary lesions. Eczema, a chronic skin condition due to atopy, drug reactions, or environmental factors, is a common cause of itch in the elderly. Excoriations secondary to scratching increase the propensity for skin infections. Elderly individuals are also pre-disposed to injury due to diminished sensory receptors. Impairment of capillary integrity can lead to recurrent purpura or bruising. Decreased barrier function enhances penetration by pathogens leading to infections. Cumulative sun exposure over lifetime can lead to photodamaged skin [Figure 2].

- Clinical image of the back of an elderly male showing cutaneous changes of photodamage characterized by multiple seborrheic keratoses, well-defined hypopigmented macules (idiopathic guttate hypomelanosis), and ill to well-defined hyperpigmented macules on the background of generalized xerosis.
Solutions are not difficult for the above-mentioned problems. As bathing is one of the initial activities of daily living lost during old age; solving measures commence with regular bathing with gentle fragrance free, moisturizing bar soap or cleanser with a pH similar to that of skin (pH-5, Syndet Bar), as recommended by the American Academy of Dermatology (AAD). It is important to differentiate fragrance free versus unscented as the latter usually contains irritant chemicals to cover up the smell of other ingredients. Overzealous bathing can cause skin irritation and damage to the stratum corneum barrier. Hence, once or twice weekly bath or daily bath for 10 min can be adopted. Hot water increases skin dryness by removal of natural oils from skin surface; hence, warm water is recommended. Bath oils should be avoided as it increases the risk of slips and falls. Gentle patting of skin with a soft cloth to leave the skin moist and application of creamy fragrance-free moisturizer within 3 min of bathing is recommended to ease dryness.[3] Environmental humidity also determines xerosis’s severity and both too-low and too-high moisture contents are detrimental with optimal range between 45% and 60%.[4] Heating and air conditioning strip humidity from air and cause dryness and itching. Using gloves while working outdoors like gardening prevent exposure to allergens and reduce the chances of skin injuries. Sun-protection measures include seeking sunshade while outdoors, especially between 10 am and 2 pm, wearing protective clothing (lightweight long-sleeved shirt, pants, wide-brimmed hat, and sunglasses with UV protection), and applying broad-spectrum water-resistant sunscreen of SPF value at least 30 to all exposed areas. Sun protection prevents dryness and photodamage. The importance of healthy diet with adequate hydration cannot be understated. Premalignant or malignant lesions develop more frequently in the elderly and it is advisable to remain observant and perform regular self-skin examination. One should not hesitate visiting a dermatologist if a new unusual spot develops or a previous one changes in size/color or bleeds/itches.
HAIRS
With age, hairs become gray and rate of hair growth decreases. In addition, the structure of hair fiber includes diameter, curvature, structural properties (rigidity and bending), and lipid composition changes, resulting in change in overall appearance of hair. Age-related lipid changes affect hair greasiness, shine, softness, and smoothness. Senescent alopecia is defined as “non-androgen-dependent hair thinning found in those over 60 years with no history of baldness in family.”[5]
For general care, AAD recommends washing of hair according to oil production by the scalp. As scalp of elderly individuals produces less oil, less frequent washing may be required. The presence of flakes warrants proper shampooing of the scalp. During washing, shampoo should be concentrated on the scalp rather than hair length and conditioning of hair is recommended after every shampoo. While going for swim, hair should be protected from the harmful effects of chlorine by wetting and conditioning hair. Tight-fitting swim caps are also recommended during swimming.
NAILS
In nails, there may be change in structure leading to platonychia or koilonychia or increased prominence of longitudinal ridges. Nails may appear dull and opaque with color varying from yellow to gray. The lunula may not be visible. “Neapolitan nails” are white nails of old age, resembling three bands as in Neapolitan ice cream, although these changes occur without any protein, liver, or kidney abnormalities.[6] Repeated trauma to untrimmed distal nail may result in transverse leukonychia. Likewise repeated trauma from footwear can result in frictional longitudinal melanonychia. The fingernails become soft and fragile and pre-disposed to longitudinal fissuring and splitting into layers while toenails become thicker (onychauxis or pachyonychia) and harder, with hyperkeratotic lesions in the toenail region. Age-related ingrowing of toenails may also occur. The prevalence of onychomycosis also increases with age.
It is good practice to keep nails clean and dry and regularly trim straight across using sharp nail scissors or clippers. Keeping nails short prevents trauma and injury. Rounding the nails slightly at the tips helps in maximizing strength. Emery board can be used to file the nails to keep them free of snags. If toenails are thick and difficult to cut, warm salt water can be used to soak feet for 5–10 min. In case of ingrown toenail, one should consult dermatologist and avoid “digging out” ingrown toenails, especially if they are infected and sore. Shoes should be proper fit and it is better to use alternate pair of shoes every day.
CONCLUSION
Proper bathing and post-bathing care form basis of skin care. Maintenance of ambient temperature and humidity ensures well-being while photoprotection will protect from solar damaged skin and/or malignancies. For hair, adequate washing and protection from harmful chemicals are essential. Keeping nails clean, dry, and trim as well as avoiding tight-fitting footwears ensures healthy nails. The importance of adequate diet and timely visit to specialist in need cannot be understated. To conclude, skin care in the elderly requires special attention as well as intention and if they are properly managed, age will prove to be just a number!
“The gray hair of experience is the splendor of the old.” Let’s prove it true!
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Dry skin in the elderly: Complexities of a common problem. Clin Dermatol. 2011;29:37-42.
- [CrossRef] [PubMed] [Google Scholar]
- Impairments in skin integrity. Nurs Clin North Am. 2017;52:405-17.
- [CrossRef] [PubMed] [Google Scholar]
- A daily skincare regimen with a unique ceramide and filaggrin formulation rapidly improves chronic xerosis, pruritus, and quality of life in older adults. Geriatr Nurs. 2018;39:24-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of environmental humidity and temperature on skin barrier function and dermatitis. J Eur Acad Dermatol Venereol. 2016;30:223-49.
- [CrossRef] [PubMed] [Google Scholar]
- A comment on the science of hair aging. Int J Trichology. 2018;10:245-54.
- [CrossRef] [PubMed] [Google Scholar]




