
Translate this page into:
The curse of the patients who feels no pain – A case report

*Corresponding author: C. K. Sriram, Department of Dermatovenereology, Velammal Medical College and Research Institute, Madurai, Tamil Nadu, India. cksriram49@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sriram CK, Krishnamoorthy A, Sundaramoorthy K. The curse of the patients who feels no pain – A case report. CosmoDerma 2023;3:49.
Dear Sir,
A 6-year-old hyperactive boy was brought by his parents for complaints of recurrent ulcers in the extremities for the past 3 years. He was the first child born to third-degree consanguineous parents. He was born by full-term normal vaginal delivery. The antenatal period was uneventful. His parents noticed delayed milestones. There was a history of recurrent episodes of fever since 2 years of age. There was no similar illness in his family members. Pedigree chart is shown in [Figure 1]. They noticed that he did not respond to any painful stimuli. They also noticed self-mutilating behavior such as biting his tongue and hitting the wall. Cutaneous examination revealed xerosis and multiple atrophic scars over his knee and leg [Figure 2a]. There were fissures in both palms [Figure 2b] and soles. Clubbing was seen in all fingers [Figure 2c]. The right sole showed a deep ulcer measuring 2 × 2 cm in the ball of the great toe [Figure 2d]. Oral cavity showed loss of the tip of the tongue, dental caries with missed tooths, and angular cheilitis [Figure 3a and b]. Sensory examination showed complete loss of sensation to pain and temperature. The fine touch and vibration sensations were intact. Deep tendon reflexes were normal. There were no hypopigmented patches in the body and enlarged or palpable nerves. A skin biopsy was denied and not done. Hematological and biochemical investigations including serum uric acid levels were normal. Based on the clinical feature and history given by his parents, a final diagnosis of congenital insensitivity to pain with anhidrosis (CIPA) was made. The ulcers were treated with antibiotics and dressings. The xerosis was managed with moisturizers and emollients. The parents were counseled about the nature of the disease and proper instructions were given.
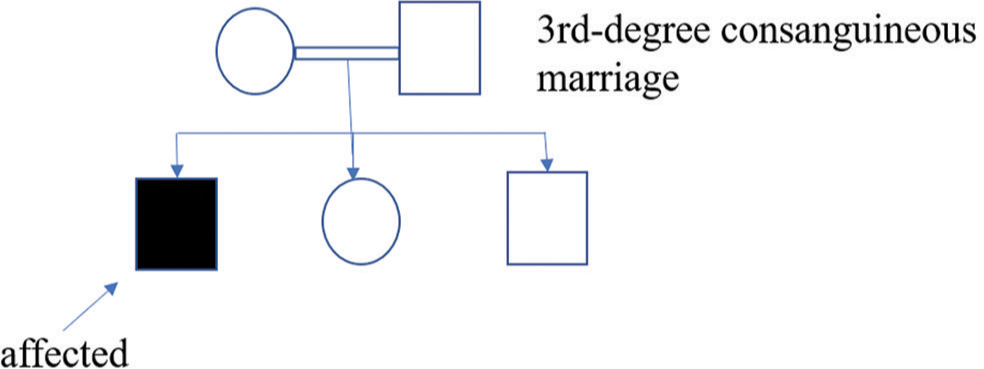
- Pedigree chart.

- (a) Multiple atrophic scars and xerosis, (b) fissures over both palms, (c) clubbing in all fingers, and (d) trophic ulcers on both soles.

- (a) Angular cheilitis and split tongue and (b) missed tooth and dental caries.
CIPA is caused by mutations in the NTRK1 gene, located on chromosome 1. This gene encodes tyrosine kinase receptors for nerve growth factors. Mutations in this gene result in the failure of differentiation and migration of neural crest cells, leading to the complete absence of small myelinated and unmyelinated nerve fibers. Hence, there is a complete loss of pain and temperature sensations. Sweat glands are also de-innervated, leading to anhidrosis.[1]
The first manifestation of CIPA is considered to be recurrent episodes of unexplained fever.[2] The common features noted are anhidrosis, mental retardation, insensitivity to pain, self-mutilating and aggressive behavior, multiple fractures, joint dislocations, and deformities. In 20% of cases, there is a chance of death in the first 3 years because of pyrexia. Insensitivity to pain results in deep ulceration on the knees and elbows, and overuse of bones and joints leading to fractures, osteomyelitis, joint dislocations, and joint deformities. Self-inflicted injuries will be in the form of skin ulcers, burns, bone fractures, autoamputations of the fingertips, and tongue.[3]
Due to anhidrosis, there will be xerosis, the thick and calloused appearance of the skin with lichenification, and fissuring of palms.[2]
Oral manifestations include ulcers on the ventral surface of the tongue due to repeated biting during infancy and causes absent tip of the tongue. Multiple missing teeth due to autoextraction may be seen in about 50% of patients.[2,3]
Histology shows normal skin and appendageal structures and the absence of non-myelinated and small-myelinated nerve fibers with preservation of sweat glands that lack innervation by small-diameter neurons.
CIPA is a painless disorder but can have devastating effects. There is no specific treatment for this condition. They must be monitored to prevent injuries, burns, fractures, and self-mutilation. The parents need to be educated about simple measures such as avoiding excessive wrapping, preventing dehydration, and measures to reduce hyperpyrexia.
Apart from the constant feature so far discussed in the literature, our patient had clubbing in all fingers as an unusual feature. The pulmonary function test was normal. There were no references or scientific reason to explain the cause of clubbing, and further, research was needed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- An infant with primary tooth loss and palmar hyperkeratosis: A novel mutation in the NTRK1 gene causing congenital insensitivity to pain with anhidrosis. Paediatrics. 2003;112:237-41.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital insensitivity to pain with anhidrosis (CIPA) Egypt Dermatol Online J. 2007;3:5.
- [Google Scholar]
- Congenital insensitivity to pain with anhidrosis. Indian J Paediatr. 2003;70:109-11.
- [CrossRef] [PubMed] [Google Scholar]




