
Translate this page into:
Premature graying of hair: A concise review

*Corresponding author: Bhushan Madke, Department of Dermatology, Venereology and Leprosy, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India. drbhushan81@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh R, Madke B, Bansod S, Yadav N. Premature graying of hair: A concise review. CosmoDerma 2021;1:65.
Abstract
Authors have attempted to provide a short concise and clinically relevant review on premature graying of hairs with the focus of updated pathogenesis, rational investigations, and treatment options. Premature graying of hairs is a fairly common clinical condition faced by dermatologists, however, very scarce therapeutic options are available for successful management of gray hairs. The role of antioxidants is not yet established firmly in the therapeutic armamentarium of premature graying of hairs. Authors have summarized the currently available therapeutic options for the treatment of premature graying of hairs.
Keywords
Premature graying
Canities
Management
Pathogenesis

INTRODUCTION
Hair, rightly called the crown of the body, plays an instrumental role in maintaining a positive societal and self-perception of an individual. Gray hair is usually associated with physiological aging, and often seen as a sign of senescence. For this reason, graying of hair prematurely can adversely affect the self-esteem of young individuals, especially the ones with darker hair type due to easy visibility of gray hair because of high contrast, where few gray strands tend to be immediately noticeable.
Hair graying is either physiological or pathological, the latter being premature most of the time. There is a definite racial variation in the occurrence of physiological aging. The traditional 50/50/50 rule of hair graying says that by the age of 50 years, 50% of the population will have 50% black hair. In a more recent large survey, however, Panhard et al. reported that only 6–23% of the people have 50% hair by the age of 50 years.[1]
The term premature hair graying (PHG) is generally used in different literature reviews when the onset of graying is before the age of 20–25 years in Caucasians, 25–30 years in Asians including Indians, and late 30’s in Blacks. PHG is determined by genetic factors, i.e., hypothesized to be inherited as an autosomally dominant trait,[2] environmental factors, and can also be seen in nutritional disorders, or pathological conditions such as osteopenia, cardiac disorders among others. Quite a few genetic, acquired and autoimmune disorders are also associated with canities.
Even with the increasing understanding of pathogenesis and ultrastructure of graying hair, the exact underlying cause for its premature onset is not very well understood, and hence a satisfactory treatment for its reversal as of today seems elusive.
ETIOPATHOGENESIS
Normal hair pigmentation
Hair color in humans is due to a process of melanogenesis in melanocytes and the distribution of pigment-containing melanosomes to the connected keratinocytes. During this process, there is synthesis of brown-black pigment called eumelanin and red-yellow pheomelanin in varied proportions. The diversity of hair color as a spectrum from black to blonde or red in different races depends on the quantity and ratio of eumelanin and pheomelanin produced.[3]
The hair follicle melanin unit consists of one melanocyte connected to five keratinocytes in the hair bulb and one melanocyte to one keratinocyte in the basal layer of the hair bulb matrix. This is in contrast to the epidermis, where the ratio of melanocytes and keratinocytes is 1:36.[4] Melanocytes are derived from the neural crest and as they move into the hair follicle, they become either DOPA oxidase-positive cells expressing tyrosinase, or DOPA oxidase negative cells, depending on which compartment they land in. The melanocytes that land in the bulb of anagen hair express tyrosinase and are melanized. The ones that land in the outer root sheath (ORS) of the hair follicle are not melanized. The amelanogenic or non-melanized melanocytes serve as stem cells, which replace the melanogenic melanocytes when they get depleted.[5]
The melanogenesis of the hair follicle is directly linked to the hair growth cycle- melanin synthesis starts at the early anagen phase, subsequently reaches its peak, and starts switching off as it reaches the catagen phase. No melanin synthesis occurs in the telogen phase. The process of melanogenesis employs three key enzymes: tyrosinase, gp75, and dopachrome tautomerase,[4] which also decline as the hair follicle moves from anagen to telogen phase. In the anagen phase of the next hair cycle, melanocytes kickstart the process of melanogenesis again.
Neuroendocrine factors also play an important role in hair melanin synthesis. ACTH, alpha melanocyte-stimulating hormone (MSH), and thyroid hormones regulate and modulate the process of melanogenesis. At the molecular level, different genes and signaling pathways have been shown to influence hair pigmentation. Receptors for bone morphogenic protein (Bmpr2), activin (acvr2a), notch signaling pathway, and stem cell factor (and its receptor kit) have been implicated to play certain different roles in hair pigmentation.[6]
Pathogenesis of gray hair
Physiological or senile canities is thought to occur due to depletion of the regenerative capacity of hair pigment cells. On average, a hair bulb undergoes 7 ± 15 cycles of melanocyte replenishment from the ORS reservoir till the age of 40–45 years after which the regenerative capacity is lost leading to hair graying.[4]
Histologically, pigmentary unit of the hair follicle is a pear-shaped structure at the tip of the dermal papilla in the pigmented hair [Figure 1], whereas in gray hair, it becomes fuzzy with diminished oligodendritic melanocytes also showing a reduced DOPA reaction with less and progressively reducing melanogenic melanocytes.[7]
PHG is likely to be due to early loss of melanogenic melanocytes, and/or defective transfer of melanosomes from melanocytes due to a variety of factors. The most important of those factors is hypothesized to be oxidative stress due to free radical generation. Oxidative stress not only promotes the differentiation of amelanogenic melanocytes to the melanogenic ones, causing a loss of regenerative capacity, but it also causes premature apoptosis of melanocytes present in the hair bulb.[8]
The free radical generation can be due to both exogenous or endogenous stress. Release of free radicals during the process of melanogenesis and as a by-product of high metabolic activity during anagen phase are the main sources of endogenous free radicals. This combined with exogenous stress from smoking, environmental damage, and psychological stress contributes to the free radical theory of graying.[9]
Dysregulation of antioxidant mechanisms in hair follicles also seems to play an instrumental role in increasing the oxidative stress. Non pigmented hair follicles have a suppressed catalase activity and decreased ferric reducing capacity.[10,11]
Patients with PHG have high oxidative stress in the hair follicle as well as in the serum, which may explain the association of PHG with coronary heart diseases.
Associated factors
Family history
In a cross-sectional, case-controlled study conducted by Sharma et al., family history of PHG was noted in 65.83% of the subjects.[2] Daulatabad et al. reported family history of PHG in 75% of the cases with an equal prevalence on both maternal and paternal sides.[12] Shin et al. found a paternal family history of PHG in 33% and a maternal family history in 11.2% of the respondents with PHG.[13] Family history and male sex are independent predictors of severity of PHG.
Smoking
In a meta-analysis, significant association was found between smoking and PHG.[14] Smoking is a well-known exogenous cause of free radical generation and oxidative stress causing premature aging changes in hair follicles.
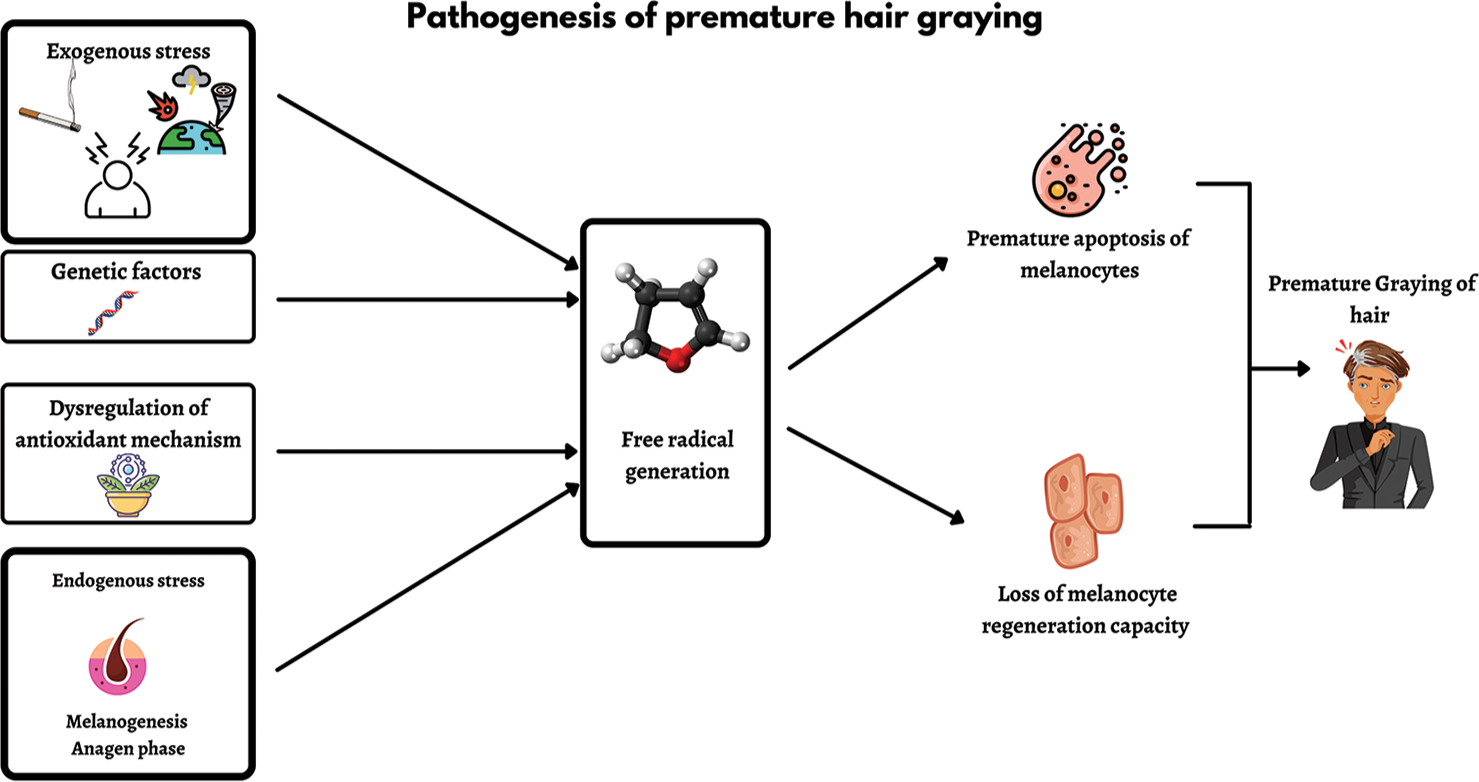
- Pathogenic factors involved in the premature graying of hair.
Metabolic risk factors
Kocaman et al. found hyperlipidemia to be an independent predictor of PGH.[15] Shin et al., in their questionnaire study, found a significant association between obesity and PGH.[13] Paik et al. also arrived at a similar finding where higher mean waist circumference was reported in the PGH group as compared to controls.[16]
Positive association between severity of hair graying and coronary artery disease (CAD) has been reported. Copenhagen City Heart study reported association of graying hair and myocardial infarction (MI) in men with a relative risk of 1.9 from their secondary data analysis.[17]
Osteopenia
Rosen reported that individuals with PGH were 4.4 times more likely to have osteopenia than individuals without PGH. However, Morton et al. in the Rancho Bernardo study, and subsequently Agarwal et al., found no significant association between PHG and bone mineral density.[18-20]
Nutritional deficiency
Various minerals act as cofactors in different phases of melanogenesis, thus their deficiencies could prematurely trigger the canities. Conversion of L-tyrosine to levodopa is mediated by tyrosinase, which is a copper-dependent enzyme and also needs calcium for phosphorylation and activation. Apart from calcium and copper, PGH is also reported with a deficiency of ferritin and zinc.[14]
Amongst Vitamins, Vitamin B12 deficiency has been found to have the most significant association with PGH. Vitamin B7 and folic acid deficiency have also been reported in patients with PGH, but it needs further corroboration.[14]
Atopy
Acer et al. reported that history of atopy is significantly higher in patients with PHG.[21] Similar findings were also reported by Daulatabad et al. in study with Indian patients where 36.5% of PHG cases had atopic diathesis, as compared to only 9% in the control group.[12]
Drugs
PHG has also been reported as a side effect of drugs like Chloroquine, Hydroxychloroquine, Imatinib (and other c-kit inhibitors), interferon, antiepileptic agents (phenytoin and valproate), tamoxifen among many others. Drug-induced hair graying is reversible in most cases by dose reduction or elimination of the offending agent.[14]
Genetics disorders
Leon et al. reported that premature onset of gray hair is seen in individuals carrying TERT mutation (human gene encoding protein component of telomerase).[22] Many rare genetic syndromes like Waardenburg syndrome, Vogt Koyanagi Harada syndrome, Werner Syndrome etc. are also associated with loss of hair pigmentation.
CLINICAL FEATURES
The mean age of onset of PHG in a case control study by Sharma et al. was 13.8 ± 4.68 years with a range of 2–22 years, and earliest age of onset being 2 years.[2] Daulatabad et al. reported the mean age of onset 11.6 ± 3.6 years, a range of 3–18 years, and the youngest case was 3 years old.[12]
Sharma et al. reported a diffuse involvement in a majority of cases (95%) with only frontal greying in 4% and only temporal greying in less than 1% of the cases.[2] All the patients in the study by Daulatabad et al. had a diffuse greying at presentation. The onset of greying was first noticed in the frontal area by 48.1% of the cases, followed by vertex in 34.6%, occiput in 13.5%, and temporal in 3.8% of the subjects. Earliest affected areas of the scalp are temporal area which are followed by the frontal and vertex areas, last to involve is the occiput.[12]
Non pigmented hair grows faster than pigmented hair. Gray hair is coarser, thicker, and more prone to weathering. The white color in canities is an optical illusion. Interaction of incident light with keratin, which is pale yellow in color, gives rise to this color.[3]
INVESTIGATIONS
Premature graying of hair is usually a clinical diagnosis, but few investigations like serum Vitamin B12, folic acid, and thyroid profile need to be performed in patients with early age of onset, without any family history.[3]
TREATMENT
PGH is a difficult to treat condition with no effective treatment option available at present. Various authors have tried quite a few different treatment options with inconsistent or no results. With ever increasing cases of canities, commonly prescribed medications are multivitamin and mineral cocktail tablets, which have no scientific evidence of efficacy.
High-dose p-aminobenzoic acid (PABA) has been tried in canities in various studies. One study mentioned giving 100 mg PABA 3 times daily produced visible improvement in the form of hair darkening which relapsed quickly within 2–4 weeks of stopping treatment.[23] Calcium pantothenate has also been found to be effective in a study conducted by Pasricha[24] on the other hand, there are also contrasting studies in the literature mentioning no results with PABA and calcium pantothenate.[25]
Pavithran found positive results of PUVASOL in premature graying of hair with complete repigmentation in 45% of the cases.[26] Bellandi et al. observed reversal of gray hair in patients who were on latanoprost for a long duration of time.[27] Sakhiya et al. reported repigmentation of gray hair following the use of 5 % melitane.[28] Melitane is a biomimetic peptide, agonist of alpha-MSH. It acts through binding melanocortin 1 receptor and thus stimulating the process of melanogenesis in hair. Palmitoyl tetrapeptide-20 is also another alpha-MSH biomimetic peptide. Studies have also shown its a beneficial role in promoting hair pigmentation and reversing gray hair.[29]
As there is no effective topical or oral treatment available, other treatment options such as plucking of gray hair and the use of hair colorants to camouflage gray hair play an essential role. Hair color can be classified as natural or synthetic. Natural hair colors usually contain Indian gooseberry, false daisy, and Henna which are mostly safe to apply but need regular touch-ups due to weak colorants.
Synthetic hair dyes are of two types: Oxidative and nonoxidative. Oxidative dyes include permanent, semipermanent, and auto-oxidative dyes. These are the most preferred type of hair colors due to longer color retention and ease of application. These dyes can easily penetrate the hair cortex while the non-oxidative dyes have the capacity to bind the keratin but are not able to penetrate the cortex.[30]
Irritant dermatitis and contact allergic dermatitis are two commonly encountered side effects of hair dye. P-phenylenediamine is the most common allergen responsible for these dermatitis.[31] A meta-analysis has showed a significant risk of developing ovarian cancer, brain tumor, and hematopoietic cancers in people using hair dye.[32] Zhang et al. have reported that permanent hair dye is more hazardous as compared to semi-permanent hair dye.[33]
Anti-aging compounds such as green tea, polyphenols, selenium, copper, phytoestrogens, melatonin are under study for their potential use in the premature graying of hair.[6] It has been seen that recombinant human growth hormone has led to improvement in not only hair growth and thickness but also in darkening of hair in some cases.[23] SkQs comprising of an antioxidant plastoquinone has been found to play a role in inhibiting the development of age-related disorders such as cataract, retinopathy, glaucoma, balding, canities, and osteoporosis in animals.[34] This molecule can also be of help in treating premature graying of the hair occurring due to oxidative stress. Topical liposomal delivery of melanin into hair follicles has also shown encouraging results.[6] An insight into the treatment options available for treatment of gray hair is given in Table 1.
| Sr. No. | Treatment of gray hair |
|---|---|
| 1. | Oral
|
| 2. | Topicals
|
| 3. | Procedural
|
CONCLUSION
Premature graying of hair has a significant psychological impact. Therefore, a long lasting and effective treatment is the need of hour. The future treatment focuses towards factors that reduce oxidative stress and accelerate melanocyte growth. Further research is needed regarding treatment modalities targeting genes and proteins that are involved in hair follicle melanogenesis.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Greying of the human hair: A worldwide survey, revisiting the “50” rule of thumb. Br J Dermatol. 2012;167:865-73.
- [CrossRef] [PubMed] [Google Scholar]
- Association of epidemiological and biochemical factors with premature greying of hair: A case-control study. Int J Trichol. 2018;10:211-7.
- [CrossRef] [PubMed] [Google Scholar]
- Premature greying of hair. Indian J Dermatol Venereol Leprol. 2013;79:641-53.
- [CrossRef] [PubMed] [Google Scholar]
- Greying: Gerontobiology of the hair follicle pigmentary unit. Exp Gerontol. 2001;36:29-54.
- [CrossRef] [Google Scholar]
- Melanocyte subpopulation turnover during the human hair cycle: An immunohistochemical study: Melanocytes during the human hair cycle. Pigment Cell Res. 2000;13:253-9.
- [CrossRef] [PubMed] [Google Scholar]
- Premature greying of hair: Review with updates. Int J Trichol. 2018;10:198-203.
- [CrossRef] [PubMed] [Google Scholar]
- Towards a “free radical theory of greying”: Melanocyte apoptosis in the aging human hair follicle is an indicator of oxidative stress induced tissue damage. FASEB J. 2006;20:1567-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of oxidative stress and psychoemotional status in premature hair greying. J Cosmet Dermatol. 2020;19:3403-7.
- [CrossRef] [PubMed] [Google Scholar]
- Premature greying as a consequence of compromised antioxidant activity in hair bulb melanocytes and their precursors. PLoS One. 2014;9:e93589.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of oxidative stress in patients with premature canities. Int J Trichol. 2015;7:91-4.
- [CrossRef] [PubMed] [Google Scholar]
- Profile of Indian patients with premature canities. Indian J Dermatol Venereol Leprol. 2016;82:169-72.
- [CrossRef] [PubMed] [Google Scholar]
- Association of premature hair greying with family history, smoking, and obesity: A cross-sectional study. J Am Acad Dermatol. 2015;72:321-7.
- [CrossRef] [PubMed] [Google Scholar]
- Premature greying of hair: Risk factors, co-morbid conditions, pharmacotherapy and reversal a systematic review and meta-analysis. Dermatol Ther. 2020;33:e13990.
- [CrossRef] [Google Scholar]
- The degree of premature hair greying as an independent risk marker for coronary artery disease: A predictor of biological age rather than chronological age. Anadolu Kardiyol Derg. 2012;12:457-63.
- [CrossRef] [Google Scholar]
- Association between premature hair greying and metabolic risk factors: A cross-sectional study. Acta Derm Venereol. 2018;98:748-52.
- [CrossRef] [PubMed] [Google Scholar]
- Gray hair, baldness, and wrinkles in relation to myocardial infarction: The Copenhagen city heart study. Am Heart J. 1995;130:1003-10.
- [CrossRef] [Google Scholar]
- Premature greying of hair is a risk marker for osteopenia. J Clin Endocrinol Metab. 1994;79:854-7.
- [CrossRef] [PubMed] [Google Scholar]
- Premature greying, balding, and low bone mineral density in older women and men: The Rancho Bernardo study: The Rancho Bernardo study. J Aging Health. 2007;19:275-85.
- [CrossRef] [PubMed] [Google Scholar]
- A study of association of premature greying of hair and osteopenia in north Indian population. Int J Trichol. 2020;12:75-8.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between diet, atopy, family history, and premature hair greying. J Cosmet Dermatol. 2019;18:665-70.
- [CrossRef] [PubMed] [Google Scholar]
- Subclinical lung disease, macrocytosis, and premature greying in kindreds with telomerase (TERT) mutations. Chest. 2011;140:753-63.
- [CrossRef] [PubMed] [Google Scholar]
- Pharmacologic interventions in aging hair. Clin Interv Aging. 2006;1:121-9.
- [CrossRef] [PubMed] [Google Scholar]
- Successful treatment of gray hairs with high dose calcium pantothenate. Indian J Dermatol Venereol Leprol. 1981;47:311-3.
- [Google Scholar]
- Effect of calcium pantothenate and para-aminobenzoic acid on the gray hair of humans. Exp Biol Med (Maywood). 1943;53:47-9.
- [CrossRef] [Google Scholar]
- Puvasol therapy in premature greying of hair. Indian J Dermatol Venereol Leprol. 1986;52:74-5.
- [Google Scholar]
- Repigmentation of hair after latanoprost therapy. J Eur Acad Dermatol Venereol. 2010;25:1485-7.
- [CrossRef] [PubMed] [Google Scholar]
- Case report on premature hair greying treated with melitane 5% and oral hair supplements. Indian J Pharmacol. 2019;51:346.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of an agonist ofα-MSH the palmitoyl tetrapeptide-20, in hair pigmentation. Int J Cosmet Sci. 2018;40:516-24.
- [CrossRef] [PubMed] [Google Scholar]
- Therapeutics of premature hair greying: A long journey ahead. J Cosmet Dermatol. 2019;18:1206-14.
- [CrossRef] [PubMed] [Google Scholar]
- Contact allergy to common ingredients in hair dyes. Contact Dermatitis. 2013;69:32-9.
- [CrossRef] [PubMed] [Google Scholar]
- Personal use of hair dyes and risk of cancer. JAMA. 2005;293:2516.
- [CrossRef] [PubMed] [Google Scholar]
- Personal use of hair dye and the risk of certain subtypes of non-Hodgkin lymphoma. Am J Epidemiol. 2008;167:1321-31.
- [CrossRef] [PubMed] [Google Scholar]
- An attempt to prevent senescence: A mitochondrial approach. Biochim Biophys Acta. 2009;1787:437-61.
- [CrossRef] [PubMed] [Google Scholar]




