
Translate this page into:
Laser safety eyewear

*Corresponding author: Deepthi Malayanur, Venkat Center for Skin and Plastic Surgery, Vijaynagar, Bangalore, India. deepu_malayanuru@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Malayanur D, Mysore VN. Laser safety eyewear. CosmoDerma 2022;2:24.
Abstract
The use of Lasers in aesthetic dermatology increased the efficacy and decreased the downtime for various dermatological procedures. In addition to the knowledge of different indications for lasers, knowledge regarding the safety precautions, and effects of lasers on human tissue is essential for the dermatologist. The safety precautions to be taken especially for eye protection need emphasis as the damage induced can be permanent. The current article deals with the effects of different laser wavelengths on eye tissue, the variety of Laser safety eyewear (LSE) available in the market, and how to read the LSE label on protective eyewear. Various LASER textbooks, UK & US national health and safety guidelines, and online LASER physics articles have been referred.
Keywords
Laser safety eyewear
Optical density
LASER goggles
Corneal shields and LSE label

INTRODUCTION
LASERs are used in dermatology for various applications. The human eye when not protected with safety eyewear is extremely sensitive to LASER radiation and can be permanently damaged from direct or reflected beams. Protection in the form of LASER glasses, LASER goggles, or LASER shields/barriers is necessary to ensure an appropriate level of protection against LASER injury. Hence insight into LASER safety eyewear (LSE) is essential for dermatologists.
The defense mechanism of the human eye against LASER is the “blink reflex” and head-turning, aversion response. The time required to close the eyelid is about 250 milliseconds and this helps for a LASER whose optical power is less than 1mW.[1] Most of the LASERs used in dermatology work in milli, nano, and picosecond scale and use optical power >1mW. Hence it is not possible for the blink reflex to protect against the damage caused by these LASERs. Also, the invisible radiation (ultraviolet, infrared) will not elicit a blink reflex to protect the eye from damage.
Laser effects on the human eye
The term LASER is an acronym for Light Amplification by Stimulated Emission of Radiation. A Laser device can emit a light beam that is monochromatic, unidirectional, minimally divergent, and coherent. The light beam emitted from such Laser devices through cornea and lens can be projected on to small point on the retina. The human eye is most vulnerable to Laser-induced damage due to this reason as most of the light either direct or reflected beam gets focused on to a small point on the retina. The eye similar to the skin has many chromophores, that is, water (cornea, lens, vitreous humor), melanin (iris and retina), and hemoglobin (choroid).[2] The cornea, lens, and retina are the most important structures of the eye that can be damaged by Laser radiation. The damage can be because of a photomechanical, photothermal, or photochemical process.[5-8]
Manifestations of eye damage due to LASERs: The symptoms of eye damage depend mainly on the wavelength of the Laser used and are summarized in Table 1 and depicted in Figure 1.
| Wavelength | Spectrum | Eye effects |
|---|---|---|
| 200-280 nm | UVC | Photokeratitis of cornea |
| 280-315 nm | UVB | Photokeratitis of cornea |
| 315-400 nm | UVA | Photochemical cataract |
| 400-780 nm | Visible | Photochemical damage to retina, retinal burn |
| 780-1400 nm | Near infrared | Cataract, retinal burn |
| 1400-3000 nm | Infrared | Aqueous flare, cataract, corneal burn |
| 3000-10,000 nm | Far infrared | Corneal burn |
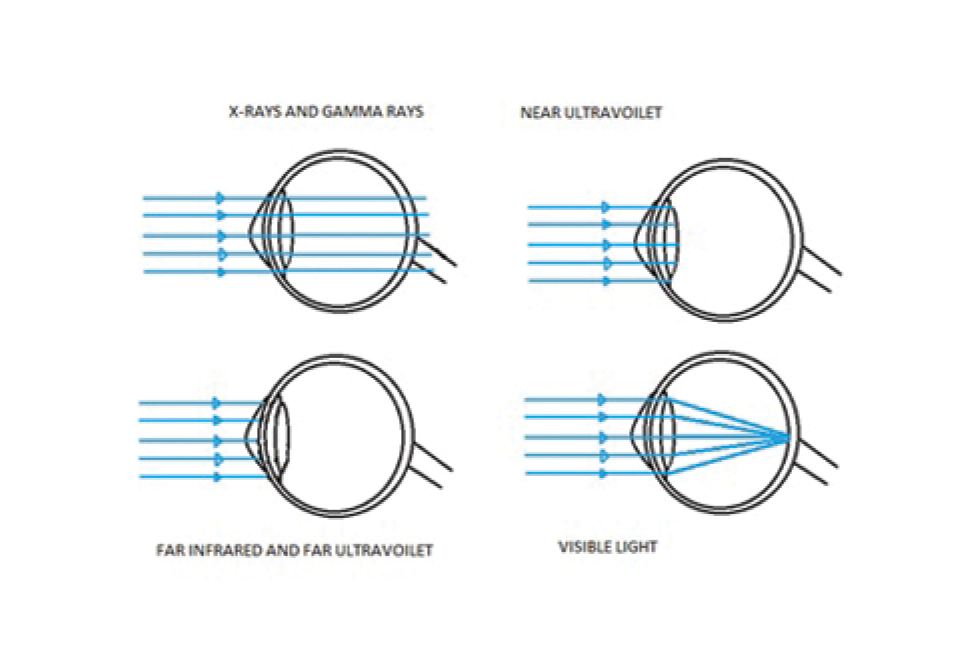
- Shows absorption of different wavelengths by eye.
When an eye is exposed to Ultraviolet light the cornea is the main target and can lead to keratitis.
When the eye is exposed to visible and near-infrared ranges (400-1400 nm), the retina is most affected. Hence this range is called Retinal Hazard Zone.[3,10-13] It causes difficulty in detecting blue or green colors secondary to cone damage. Exposure to the near-infrared range, like the Q-switched Nd : YAG LASER beam (1064 nm), can cause eye damage that may initially go undetected as it is invisible and the retina lacks pain sensory nerves. Hence it is more dangerous. The retinal damage due to Q switched can be photoacoustic and an audible “pop” can be heard at the time of exposure.[4] The visual damage may not be recognized by the LASER operator until considerable thermal damage has occurred.[5]
When the eye is exposed to far infrared range, cornea and/lens can be damaged due to its preferential absorption by water. For example, exposure to the far infrared range LASERs like invisible CO2 LASER (10,600 nm) can manifest as a burning pain at the site of exposure on the cornea or sclera. Primary eye injury can lead to secondary eye injuries that are caused by the shock wave, heat, and release of various noxious agents.[5]
Factors affecting LASER induced eye injury
The site and extent of ocular damage depends on both eye variables and laser variables.[2]
The eye variables are:
The location of damage in the eye—fovea damages are worst as this is the part of the retina with maximal visual acuity.
The color of the iris—dark-skinned ones are more affected as the amount of chromophore, that is, melanin is more.
Whether a pupil is dilated or not—the pupil is maximally dilated in dark than bright light and dilated pupil allows more amount of LASER light to pass through. Hence LASER operation in dark is more dangerous than daylight.
The refractive state of the eye at the time of injury— in the ametropic eye, the laser point of focus can be before or behind the retina, and hence the area of involvement on the retina is larger but in contrast, the irradiance is less. For example, a change in eye dioptric power by 1 D can lead to a 10-fold increase in retinal spot size but the irradiance is decreased by two orders of magnitude.[2]
The LASER variables are
Wavelength: Lasers operating at different wavelengths have varied effects on different segments of the eye as explained in Table 1.
Pulse duration: The pulse duration of most of the LASERs used in dermatology is less than the blink reflex (250 millisecond), which makes all pulse duration at risk. Shorter the pulse duration, the faster the delivery of LASER energy. Hence Q-switched LASERs cause greater damage.
Energy/fluence: The higher the LASER energy used, the greater is the risk of eye damage.
Beam diameter and spot size of the LASER. The bigger the beam diameter, the greater the damage.
Prevention of LASER induced ocular injury
The most important way of preventing of eye injury is LSE.[16] Proper eye protection should be used by the operator, staff, and patient. There are various models available in the market for the operator and patient use.
Types of LASER safety eyewear (LSE)
For operator protection:
Wraparound—Wraparound frames are the most common style. With a wide range of shapes and sizes, this style is suitable for most available filters whilst also providing a lightweight and low-profile design.
Goggles/Masks—Goggle and mask frames are used to accommodate thicker filters when a higher level of protection is required. These robust frames utilize a head strap and padding for maximum comfort.
Over spectacles—Over spectacle frames are designed to accommodate prescription glasses underneath. This style provides lots of room for most prescription frames without obscuring the field of view.
For patient protection
Goggles—These patient goggles may be made of heatproof stainless steel with an anodized convex surface without any transparency. These frames are suitable for deep blocking filters for Intense Pulsed Light (IPL) and other bright light treatments.
Corneal shields—Intraocular Laser eye shields (corneal eye shields) are designed to protect the patient’s eyes during Laser procedures and are designed to fit into the patient’s eyes, just like contact lenses. There are many types of corneal shields available in the market made of different colors and materials like polymethacrylate, metal shields, plastic shields, etc.[12,13] The metal shields are made of surgical-grade stainless steel. The outer covering of the intra-ocular eye shield is non-reflective and ideal for Laser procedures in which the ocular area or orbital rim is being treated.[14] For example, while using Q switched LASERS to treat Naevus of Oto. The eye shields when placed behind the eyelids are designed in such a way that they won’t move during the treatment. Metal eye shields can also be irritating to the eye and might leave certain parts of the eye vulnerable, such as the superior conjunctival fornix. Before inserting an eye shield, an ophthalmic topical anesthetic ointment or drops should be first applied to the eyes. Separate the patient’s eyelids and place the eye shield gently on each eye. Make sure that the eye shields are placed under both upper and lower eyelids. Intra-ocular eye shields may be sterilized via autoclave or ETO (ethylene oxide gas). Figure 2 shows different types of LSE used for LASER operation.

- Different types of LASER safety eyewear.
Factors to be considered while selecting LSE
Wavelength: There are typically two wavelengths associated with a LASER, the aiming beam wavelength and the operating wavelength. Typically, the aiming beam is “eye-safe” and the operating beam is the one that needs protection. It is emphasized that many LASERs emit more than one wavelength and that each wavelength must be considered.[7]
For example, a frequency-doubled Nd : YAG operating at 532 nm may emit about 2 watts at the green wavelength while the Nd : YAG LASER itself operating at 1064 nm in the near-infrared emits 50 watts. But some safety filters which strongly absorb the 532 nm wavelength may absorb essentially nothing at the 1064 nm wavelength.
Optical density (OD): It is the measure of LASER energy that can pass through a filter. Maximum the optical density maximum is the safety. Though ideally, OD of 10 gives maximum protection the visibility is compromised. Hence a balance between protection and visibility is considered while making goggles.
Example: OD of 4.0 allows 1/10,000 of the LASER light energy to be transmitted.
LASER beam intensity: For pulsed LASERs, the beam size is needed and intensity is expressed in radiant exposure units of (joules/cm2). For Continuous Wave LASERs measured in terms of beam irradiance (Watts/cm2).
Visible transmittance of eyewear: Since the object of LASER protective eyewear is to filter out the LASER wavelengths while transmitting as much of the visible light as possible, the visible (or luminous) transmittance should as high as possible. A low visible transmittance (usually measured in percent) creates problems of eye fatigue and may require an increase in ambient lighting. However, adequate optical density at the LASER wavelengths should not be sacrificed for improved visible transmittance.
Modes of operation of LASER: LASERs operating at different modes, as described in Table 3, have different power density characteristics and often different eyewear requirements. For example: Continuous-wave, pulsed, and mode-locked.
LASER safety guidelines
LASERs have been classified by wavelength and maximum output from class 1 to class 4. Table 2 shows the classification of Lasers.[17] Most of the LASERs used in dermatology belong to class 3B or 4. They carry a greater risk of eye damage in their applications.
| ANSI & IEC CLASS SUB-CLASS |
CLASS 1 1 1M |
CLASS 2 2 2M |
CLASS 3 3 R 3 B |
CLASS 4 |
|||
|---|---|---|---|---|---|---|---|
| Human accessible laser power | Visible light-emitting <0.39mW | Visible light-emitting <1mW | Visible light emitting1mW-5 mW | Visible light emitting5mW-0.5W | Any laser >0.5 W | ||
| Eye hazard for intraocular laser exposure | Safe even for unintentional viewing | Safe for the unaided eye. Hazardous when viewed through optical instruments | Safe for unintentional viewing, 0.25 second. | Safe for unintentional viewing, 0.25 second. Hazardous when viewed through optical instruments | Low risk for Unintentional or accidental exposure to direct or reflected light Avoid intentional viewing into beam | Eye hazard Avoid exposure to direct or reflected beam | Severe eye hazard Avoid exposure to direct or reflected beam |
| Caution on label | None | Do not view directly with optical instruments | Do not stare into the beam | Do not stare into beam and view with telescopic instruments | Caution | warning | Danger |
| Examples | Laser printers CD players | Optical fiber communication system | Laser pointers Barcode scanners | Level and orientation civil engineering instruments | Laser pointers Alignment lasers | Lasers for physiotherapy | Laser surgery devices Laser metal cutting devices |
The International Electro Technical Commission (IEC) is a global organization that prepares and publishes international standards for electrical, electronic, and related technologies.[17] The IEC document 60825-1 is the primary standard that outlines the safety of LASER products. Different nations have different local regulations based on IEC standards. LASER Safety falls under the ANSI 136.1 standard in the United States and the EN207 standard in Europe.
The American National Standards Institute (ANSI) guidelines regarding Laser safety are given in the ANSI Z136 series of standards.[18,19] The American standard for LASER safety wear only requires specification according to OD of filters.
The European LASER Safety Standards guidelines regarding Laser safety are published in EN 207 guidelines.[20] Any LASER eye protection sold within the European Community must be certified and labeled with the CE mark. The European LASER safety standards consider not only the OD but also the power/energy density of the LASER when determining LASER safety requirements in contrast to American guidelines.
The LASER beam must be prevented from reaching the eyes from the sides and the filters should form an inseparable unit with the frame. The “weaker” part determines the protection level of the whole system for the specified wavelength and operation mode. According to EN 207 both the filter and the frame must be accounted for when specifying the safety level, therefore, the lower of the two is used.
Understanding the LSE label on Laser safety eyewear
The operating doctor and staff in the Laser room should know how to choose and read the numbers on protective eyewear while performing laser procedures.
The LB number is the scale defined in the EN 207:2009 standards.[20,21] This specifies eyewear protection against LASER radiation using a glass or plastic material. The LB scale defines the minimum markings required on the LASER safety glasses to ensure protection from the specified LASER.
There are three parts to each LB rating
The first part defines the wavelength, or range of wavelengths, at which the rating is valid.
The second part, letters in front of the LB number refer to the temporal mode of the LASER beam as described in Table 3.
The final part of the CE rating is the LB rating itself. This integer value represents the maximum power that the eyewear filters protect against.
Example: The LB-rating is commonly written as below:
700-760 DIR LB 5
Where 700-760 is the wavelength range (nm) the goggle can provide protection, D is the mode of the LASER and LB5 represents protection level 5 for the LASER type at this wavelength.
The value of the LB numbers increases in attenuation magnitude as factors of 10. For example, LB2 safety goggles have ten times the attenuation of LB1 goggles. They will withstand 10 times the power density or energy density.
The minimum optical Density of the eyewear is equal to the LB number specified. For example, a rating of LB2 means that the OD is >2.
The minimum LB number in EN 207 standards is LB1. If the power or energy density of the LASER is less than 0.1 times the LB limit, it means safety eyewear might not be needed. The highest LB number is LB 10. If the power or energy density of the LASER is greater than the LB10 limit, it means the commercially available safety wear is not enough for eye protection. The protection in such scenarios is best by adapting engineering controls so that exposure to these conditions is not possible.
CONCLUSION
Most of the LASERs used in dermatology belong to Class 3 B and Class 4 which require eye protection in the form of safety eyewear. An unprotected eye is prone to damage depending on the wavelength used and the damage can be sometimes irreversible. Hence eye protection is an important topic in LASER training, LASER use, and LASER security.
DECLARATION OF PATIENT CONSENT
Patient’s consent is not required as there are no patients in this study.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICT OF INTEREST
There are no conflicts of interest.
References
- How light reaches the eye and its components. Int J Toxicol. 2002;21:501-09.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of alleged retinal laser injuries. Arch Ophthalmol. 2004;122:1210-17.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular injury in cosmetic laser treatments of the face. J Clin Aesthet Dermatol. 2018;11:15-8.
- [PubMed] [Google Scholar]
- Ocular damage secondary to lights and lasers: How to avoid and treat if necessary. World J Ophthalmol. 2014;4:1-6.
- [CrossRef] [Google Scholar]
- Lichtinduzierte schäden am auge [Light-induced damage to the eye] Fortschr Ophthalmol. 1990;87:S41-51.
- [PubMed] [Google Scholar]
- Retinal injury following laser pointer exposure. Dtsch Arztebl Int. 2017 Dec 8;114:831-37.
- [CrossRef] [PubMed] [Google Scholar]
- The safety of laser pointers: Myths and realities British. Br J Ophthalmol. 1998;82:1335-38.
- [CrossRef] [PubMed] [Google Scholar]
- Practical aspects of laser safety. Facial Plast Surg. 2001;17:155-63.
- [CrossRef] [PubMed] [Google Scholar]
- Laser safety: Risks, hazards, and control measures. Laser Ther. 2011;20:95-6.
- [CrossRef] [PubMed] [Google Scholar]
- Laser light: Its nature and its action on the eye. CMAJ. 1989;141:1141-48.
- [PubMed] [Google Scholar]
- Laser safety features of eye shields. Lasers Surg Med. 1996;18:309-15.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of corneal eye shields in protecting patients’ eyes from laser irradiation. Dermatol Surg. 1996;22:613-16.
- [CrossRef] [PubMed] [Google Scholar]
- Health Devices. 1993;22:159-204.
- [PubMed]
- Safety of laser products: Part 1-equipment classification and requirements. IEC 2014:60825-1.
- [Google Scholar]
- Z 136.3 For the Safe Use of Lasers in Health Care Facilities New York: American National Standards Institute; 2018.
- [Google Scholar]
- European EN 207 and EN 60825 Personal Protection Equipment, Laser Safety Standards: http://www.hse.gov.uk/foi/internalops/oms/2009/03/om200903app3.pdf
- Laser Safety/Eye care In: Sardana K, Garg VK, eds. Lasers in Dermatological Practice (1st ed). New Delhi: Jaypee Brothers; 2014. p. :493-501. In: editors.
- [Google Scholar]
- Laser safety (1st ed). New Delhi: Springer; 2019. p. :297-308. In: Issa MCA, Tamura B editors. Lasers, lights and other Technologies
- [Google Scholar]
- Lasers and lights for treating pigmented lesions In: Nouri K, ed. Lasers in Dermatology and Medicine, Dermatological Indications (2nd ed). Switzerland: Springer; 2018. p. :100. In: editor.
- [Google Scholar]




