
Translate this page into:
Giant plaque-like dermatofibromas presenting over an atypical site

*Corresponding author: Anita Marak, Department of Dermatology and STD, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India. anita.marak@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gurudharshane R, Marbaniang E, Marak A. Giant plaque-like dermatofibromas presenting over an atypical site. CosmoDerma. 2024;4:71. doi: 10.25259/CSDM_50_2024
Abstract
Dermatofibroma, a benign fibrohistiocytic tumor, rarely presents as atypical lesions over sites other than its usual distribution which often poses a challenge in making a clinical diagnosis. Giant dermatofibroma is one such variant, presenting with pedunculated lesions larger than 5 cm in size. A subtype of giant dermatofibroma, plaque-like dermatofibroma, manifests clinically with indurated plaques, with eight such documented cases in the past.We are reporting one such presentation over a site that has not been documented in the existing literature to date.
Keywords
Dermatofibroma
Fibrohistiocytic tumors
Benign fibrous histiocytoma

INTRODUCTION
Dermatofibroma typically manifests during middle age as a solitary, slow-growing, and circumscribed nodule over the lower limbs and trunk. One relatively uncommon clinical variant is the giant plaque-like dermatofibroma, characterized by a size exceeding 5 cm, with an obscure clinical diagnosis, due to its size and morphology. Here, we are reporting a patient with giant plaque-like dermatofibromas over both breasts.
CASE REPORT
A 38-year-old lady presented with gradually progressive itchy, hyperpigmented, and raised lesions over both breasts for three years. There was no history of redness or ulceration noted over the lesions. She did not notice any trauma before the onset, although a history of insect bite was present. The patient did not have any other comorbidity. On examination, two well-defined, discrete, hyperpigmented, and indurated plaques were noted [Figure 1], one each over the upper inner quadrants of breasts, measuring about 7 cm in diameter, with prominent hair follicles. The lesion over the left breast was seen encroaching the areola present inferolaterally. Breast examination did not reveal any abnormality.

- 38 year old woman presented with well-defined, violaceous erythematous plaque of diameter 7 cm in size, over the left breast, with prominent hair follicles. The lesion can be seen encroaching the corresponding areola inferolaterally.
Histopathologically, hyperkeratosis was noted with a circumscribed lesion in the dermis comprising of spindle cells arranged in fascicles and focal storiform pattern along with focal areas of myxoid degeneration, which was suggestive of dermatofibroma [Figure 2a and b]. Immunohistochemistry (IHC) showed cells positive for CD68 (focal positive), but negative for CD34 [Figure 3a and b]. Ultrasound of the site showed breast imaging-reporting and data system-2 – suggestive of a benign lesion. Mammography of both breasts revealed no significant abnormalities.
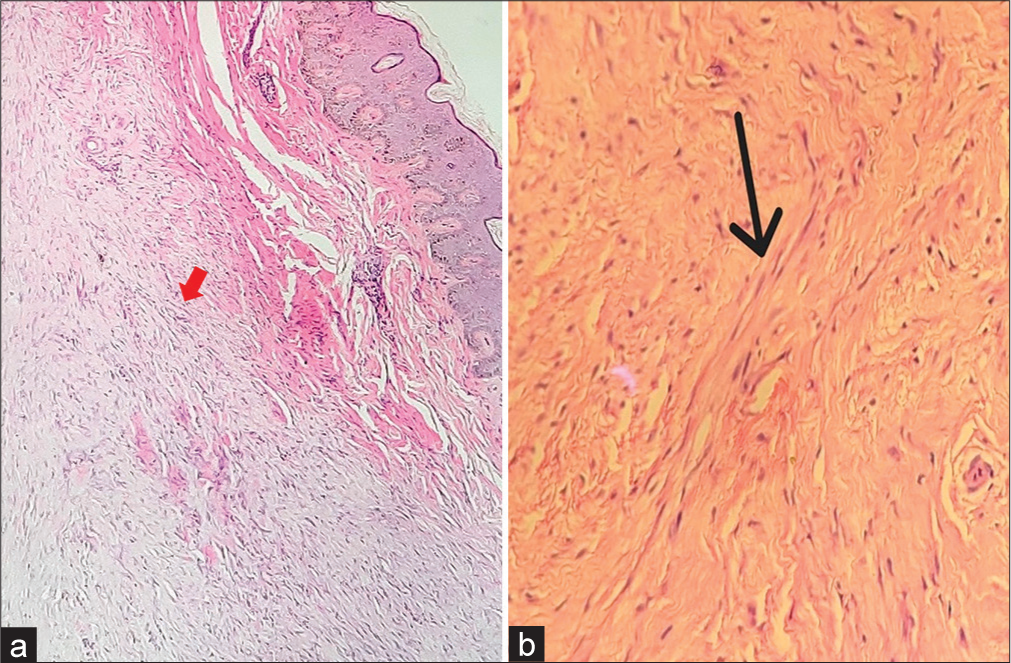
- (a) Histopathology showing hyperkeratosis with a circumscribed lesion in the dermis comprising of spindle cells arranged in fascicles denoted by red arrow. Focal areas of myxoid degeneration and epithelioid cells with abundant cytoplasm were noted amidst (H&E stain; ×40 magnification). (b) Histopathology showing focal storiform pattern denoted by black arrow. (H&E stain; ×40 magnification).
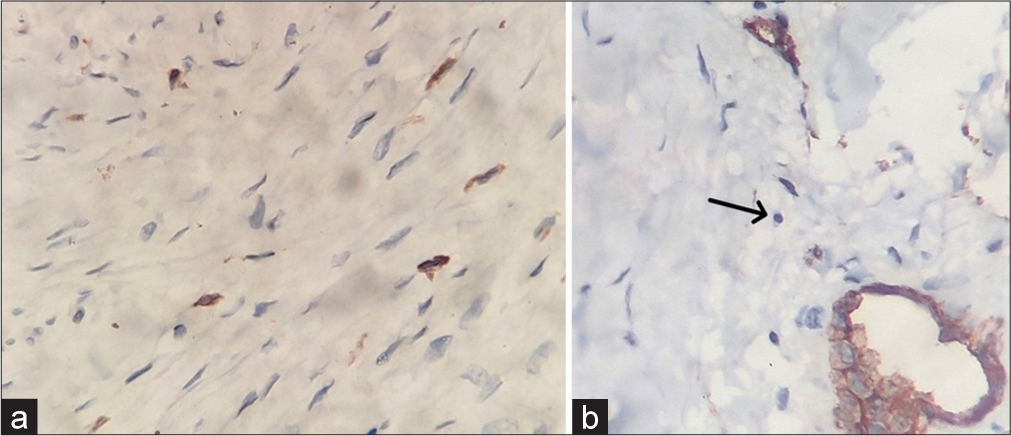
- Immunohistochemistry (IHC) showing (a) CD68 positivity in histiocytic cells (IHC stain for CD68; 40x magnification). (b) IHC negative for CD34 in cells – highlighted by black arrow; with positivity in blood vessels – control (IHC stain for CD34; ×40 magnification).
Dermoscopy was performed, which revealed the presence of a central white structureless scar-like patch with prominent pseudo-follicular openings [Figure 4a and b].
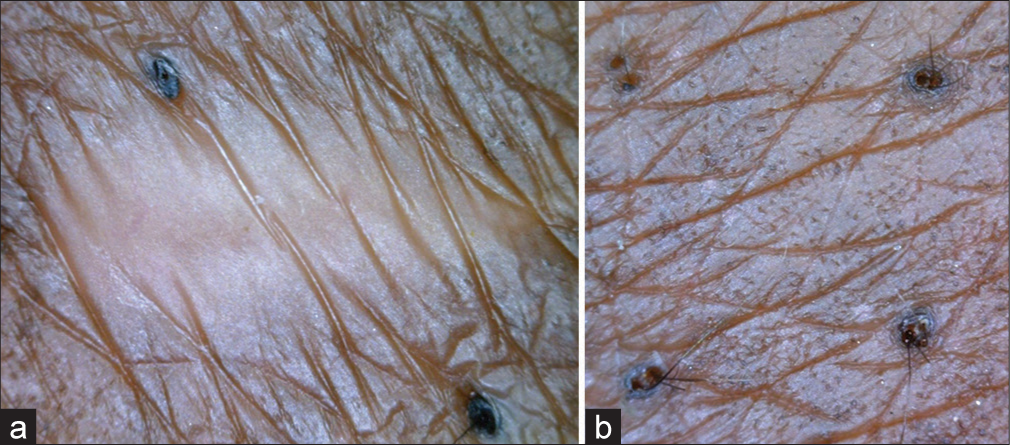
- (a) Dermoscopy showing presence of central white structureless patch. (b) Dermoscopy with prominent pseudofollicular openings in the periphery.
DISCUSSION
Several clinical variants of dermatofibroma have been reported previously: atrophic, atypical polypoid, giant, subcutaneous fibrous, multinodular hemosiderotic, keloidal, subungual pleomorphic, generalized eruptive, erosive, ulcerated, multiple palmoplantar, and multiple clustered.[1] A giant dermatofibroma, first described by Danckaert and Karassik, is defined as a dermatofibroma with a diameter of more than 5 cm in size.[2,3] It typically presents as an exophytic lesion, with a predilection to affect the lower limbs followed by the back, as concurred by a review of literature on giant dermatofibromas.[4]
Plaque-like dermatofibromas are considered a variant of giant dermatofibromas, with very few cases mentioned in the literature, presenting as large, indurated plaques that develop either spontaneously or due to trauma, such as insect bite.[5-8] Due to the size and presentation, differential diagnoses usually include malignancies such as dermatofibrosarcoma protuberans, basal cell carcinoma, epidermoid carcinoma, cutaneous lymphoma, or sarcoma.
In this patient, the unusual site and appearance prompted consideration of differential diagnoses such as cutaneous malignancies, metastases, and Bowen’s disease. However, histopathology revealed the presence of features suggestive of the common fibrous/fibrocellular variant of dermatofibroma.
Various histopathological variants have been described with both the classical and giant type of dermatofibroma, namely – common fibrous/fibrocellular, xanthomatized, aneurysmal, hemosiderotic, epithelioid, cellular, atrophic, lipidized, clear cell, palisading, keloidal, and many more.[4,9] While no studies have been conducted to date on the histopathological features of plaque-like dermatofibroma, existing literature reveals that they exhibit features similar to the common fibrous/fibrocellular variant of a typical dermatofibroma – a non-capsulated, ill-defined dermal lesion composed of interlacing fascicles of spindled cells comprising fibroblasts and macrophages. This structure is sometimes arranged in a focal storiform arrangement, set within a loose collagenous stroma.[5-8] IHC with CD68 stain highlights the presence of histiocytic cells, while the absence of CD34 rules out dermatofibrosarcoma protuberans (positive in 85% of cases) and might be the only differentiating feature. However, the cellular variant may focally stain positive for CD34, predominantly at the periphery of the tumor. Factor XIIIa is another stain that can be used to differentiate the two, as it is usually negative in dermatofibrosarcoma protuberans.[8]
Recently, dermatoscopy has been used to aid in the diagnosis of dermatofibroma. The most common pattern described is the presence of a peripheral delicate pigment network with a central white structureless scar-like patch, although various other findings such as ring-like globules, red-blue structureless areas, white streaks and blotches, peripheral vascular blush, and prominent pseudo-follicular openings can be seen, especially with other atypical clinical and histopathological variants of dermatofibroma.[10,11] The current patient showed features of a central white structureless patch and prominent pseudofollicular openings but a peripheral delicate pigment network was absent.
This case report is distinctive as it documents the first instance of giant plaque-like dermatofibromas not only occurring over an uncommon location but also presenting with bilateral symmetrical involvement of the breasts. Diagnosis is usually clinical, however in lesions with atypical presentations as seen in ours, histopathological evaluation along with IHC is helpful in accurate diagnosis and differentiation from other conditions. In addition, dermatoscopy in atypical dermatofibromas is also an essential tool in establishing a diagnosis. An initial dermatoscopic evaluation may be suggested before an invasive investigation, especially in young adults presenting with a plaque over the breast after an underlying malignancy has been ruled out by examination and relevant imaging modality.
Albeit its appearance, it invariably follows a benign course, and simple excision is found to be curative in most cases. No recurrence has been reported to date post-excision.[5]
CONCLUSION
This case report documents a rare instance of giant plaque-like dermatofibromas with involvement of bilateral breasts. Diagnosis can be challenging in such cases, thus requiring histopathological evaluation, immunohistochemistry, and dermatoscopy for accuracy.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Clinical and histological patterns of dermatofibroma without gross skin surface change: A comparative study with conventional dermatofibroma. Indian J Dermatol Venereol Leprol. 2015;81:263-9.
- [CrossRef] [PubMed] [Google Scholar]
- Giant dermatofibroma. A little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-8.
- [CrossRef] [PubMed] [Google Scholar]
- Giant dermatofibroma: Case report and review of the literature. Actas Dermosifiliogr. 2007;98:121-4.
- [CrossRef] [PubMed] [Google Scholar]
- Plaque-like dermatofibroma: A case report and review of the literature. Turk Arch Dermatol Venereol. 2022;56:190-2.
- [CrossRef] [Google Scholar]
- Plaque-like dermatofibroma with satellitosis in a young woman. Int J Dermatol. 2019;58:1199-201.
- [CrossRef] [PubMed] [Google Scholar]
- Plaque-Like dermatofibroma: Case report of a rare entity. Dermatopathology (Basel). 2021;8:337-41.
- [CrossRef] [PubMed] [Google Scholar]
- Plaque like giant dermatofibroma: A case report. J Cutan Aesthet Surg. 2017;10:51-3.
- [CrossRef] [PubMed] [Google Scholar]
- Variants of dermatofibroma--a histopathological study. An Bras Dermatol. 2014;89:472-7.
- [CrossRef] [PubMed] [Google Scholar]
- Dermoscopy of dermatofibromas: A prospective morphological study of 412 cases. Arch Dermatol. 2008;144:75-83.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple dermatofibromas: Dermoscopic patterns. Indian J Dermatol. 2013;58:243.
- [CrossRef] [PubMed] [Google Scholar]




