
Translate this page into:
Do cosmetics have a role in melasma? Preliminary results of a pilot study of patch testing in melasma

*Corresponding author: C. Divyalakshmi, Department of Dermatology, AIIMS Rishikesh, Dehradun, Uttarakhand, India. cdivya93@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Divyalakshmi C, Bhatia R, Hazarika N. Do cosmetics have a role in melasma? Preliminary results of a pilot study of patch testing in melasma. CosmoDerma 2023;3:99.
Abstract
Objectives:
Melasma can be associated with pigmented contact dermatitis (PCD) that often goes unrecognized. The concept of cosmetic contact sensitivity in melasma is relatively less studied. In this era of overwhelming use of cosmetics among both men and women, the role of various cosmetic products in melasma and PCD needs to be extensively explored. Patch test in melasma patients can help recognize this cosmetic contact sensitivity in melasma patients. Thus, our study was to find the role of cosmetics in melasma patients.
Material and Methods:
A hospital-based, pilot study conducted in the Dermatology outpatient department of All India Institute of Medical Sciences, Rishikesh, Uttarakhand from January 2020 to February 2020. Seventeen consecutive patients with melasma were patch tested with Indian cosmetic series procured from the Systopic Pharmaceutical Ltd., standard set of commercial cosmetic products and patient products, if applicable. Day 3 and 5 readings were recorded.
Results:
Patch test was positive in 15 (88.2%) patients, with a relevance of 66.7%. Thiomersal was the most common allergen (53.3%) observed in our study population.
Conclusion:
Thiomersal in cosmetic products may be an important allergen to cause melasma.
Keywords
Melasma
Patch test
Cosmetics
Contact sensitivity
Allergen

INTRODUCTION
Melasma is a common acquired condition of symmetric hyperpigmentation, typically occurring on the face, with higher prevalence in females and darker skin types.[1] An insight into the triggers of the disease is essential to plan the therapeutics that precisely aim the disease process and prevent relapses.[2] Occurrence and persistence of melasma in non-pregnant, non-lactating females, and recent rising trend, kindle minds of many researchers. Today, the use of cosmetics and skin care products has tremendously increased. Pigmented cosmetic dermatitis, as proposed by Nakayama et al.,[3] is a variant of pigmented contact dermatitis where cosmetic ingredients are the primary allergens and the face is involved predominantly. Clinically, diffuse or patchy brown hyperpigmentation occurs over cheeks and/or forehead or the entire face making its differentiation difficult from melasma.[4] However, this aspect of cosmetic contact sensitivity in melasma remains under reported. In this pilot study, we present our findings on cosmetic contact sensitivity in melasma patients by studying the role of cosmetics in melasma patients.
MATERIAL AND METHODS
A hospital-based, pilot study, conducted in the Dermatology outpatient department of All India Institute of Medical Sciences, Rishikesh, Uttarakhand from May 2019 to June 2019. After a written and informed consent, 17 consecutive patients with melasma were patch tested with Indian cosmetic series procured from the Systopic Pharmaceuticeutical Ltd., approved by Contact and Occupational Forum of India, standard set of commercial cosmetic products and patient products, if applicable. Day 3 and day 5 readings were noted and documented [Table 1]. Data were tabulated and analyzed.
| Patient number | 1+ positive | 2+ positive | 3+ positive | Irritant reaction |
|---|---|---|---|---|
| Patient 1 | Butyl hydrate, Sorbitan sesquioleate, hexamine, Fair and Lovely cream, Patanjali cream | Thiomersal | ||
| Patient 2 | Musk mix, PPD | |||
| Patient 3 | Thiomersal, musk mix, rose oil, jasmine absolute, cetyl alcohol, Germall 115, benzotriazole, benzyl salicylate, phenyl salicylate, chlorhexidine, sorbic acid | Triclosan | ||
| Patient 4 | Cetrimide, thiomersal | |||
| Patient 5 | Thiomersal, sorbic acid, hexamine, phenyl salicylate, lavender absolute, musk mix | |||
| Patient 6 | Angry back phenomenon | |||
| Patient 7 | Fair and Lovely cream, Vicco turmeric cream, Patanjali cream | |||
| Patient 8 | Phenyl salicylate, PPD | |||
| Patient 9 | Butyl hydrate, thiomersal | Himalaya face wash | ||
| Patient 10 | Himalaya face wash | |||
| Patient 11 | - | - | - | - |
| Patient 12 | Thiomersal | |||
| Patient 13 | Thiomersal | Severe tape reaction | ||
| Patient 14 | Germall II, Fair and Lovely cream, Patanjali cream | Vicco turmeric cream, Pond’s cream | Himalaya face wash | |
| Patient 15 | Thiomersal, cetrimide | |||
| Patient 16 | Cetyl alcohol, Fair and lovely cream, Himalaya face wash | |||
| Patient 17 | Phenyl salicylate, cetrimide, Fair and lovely cream, Vicco turmeric cream |
RESULTS
Seventeen cases of melasma, aged 20–46 years, were patch tested. Mean age was 34.2 years. Majority of the cases were female (n = 13, 76.4%). Mean disease duration was 39 months (2 months to 9 years). Centrofacial pattern of melasma was the most common (76.5%) followed by the malar pattern (17.6%) and 0.05% mandibular pattern. Patch test was positive in 15 (88.2%) patients, with a relevance of 66.7%. Common contact sensitizers were thiomersal (53.3%), cosmetic creams (40%), phenyl salicylate (26.7%), and cetrimide (20%) [Figure 1]. Angry back phenomenon was seen in one case [Figure 2], severe tape reaction in two cases, and irritant reaction in three cases [Figures 3-5].

- Graphical representation of the allergens tested positive in our patients.
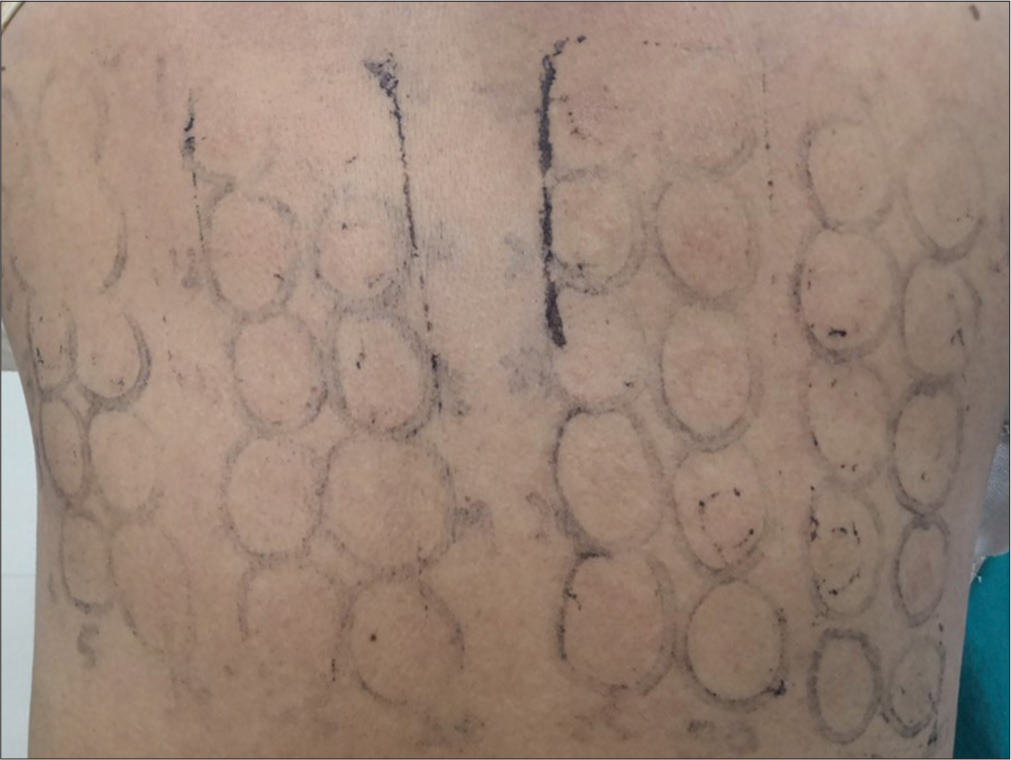
- Angry back phenomenon.

- Centrofacial melasma with relevant positive test to butyl hydrate and thiomersal (use of ponds cream).
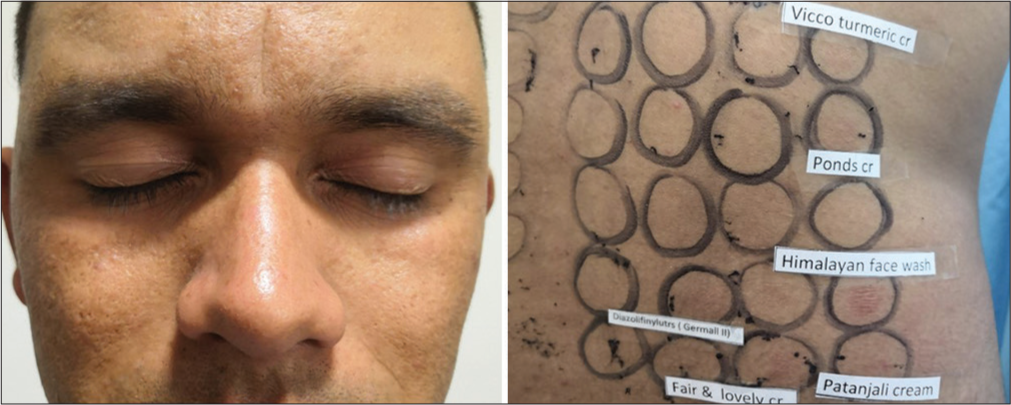
- Centrofacial melasma with relevant positive test.
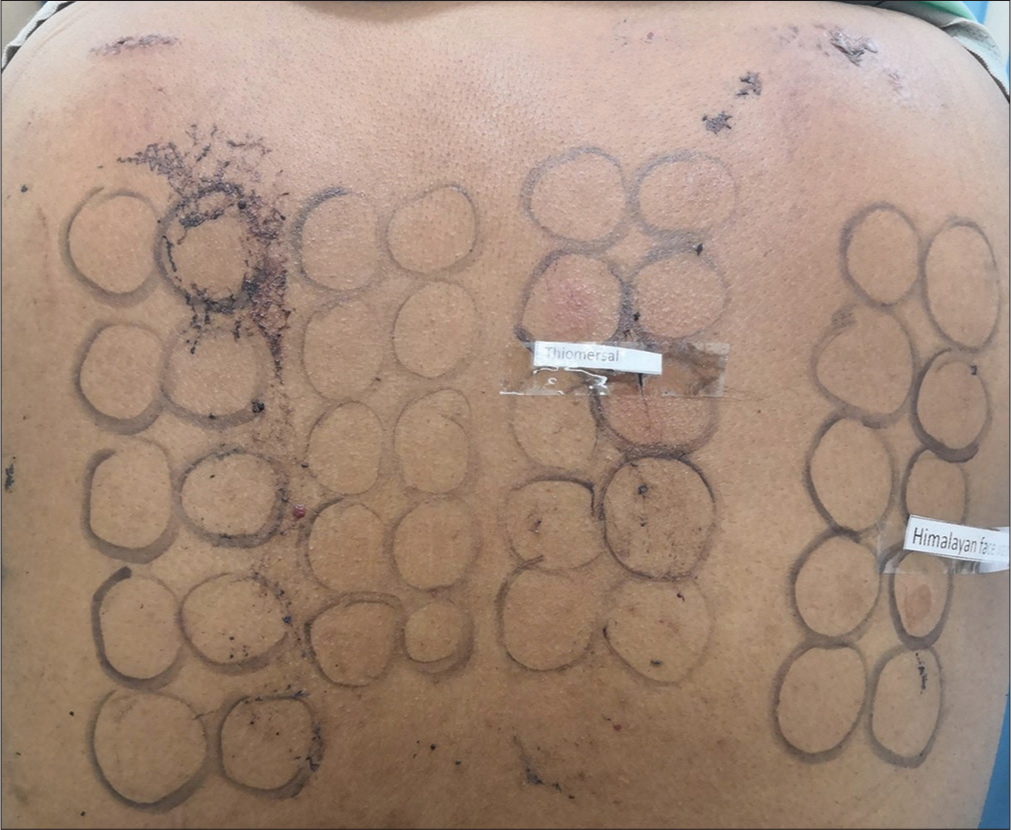
- 1+ to thiomersal and irritant reaction to Himalaya face wash.
DISCUSSION
Melasma is an acquired hypermelanosis with long-standing effect on psychology and quality of life.[4] It accounts for 0.25–4% of the patients seen in dermatology clinics in South East Asia and is also a common pigmentary disorder among Indians.[5,6] Genetic predisposition, pregnancy, oral contraceptives, endocrine dysfunction, hormone treatments, or exposure to UV light are the most implicated etiologic factors in melasma.[7] Cosmetics have been rarely considered in causation of melasma. Thiomersal, an organic mercury compound used as preservative in many cosmetics, was the most common allergen tested positive in this study [Figure 5]. In a similar study by Prabha et al.,[4] cetrimide was the most common allergen followed by gallate mix and thiomersal with positive reaction in patients using fairness cream. Mercury is a rarely listed ingredient in many cosmetic products. Al-Saleh et al.[8] analyzed “Fair and Lovely” fairness cream and found traces of mercury that was otherwise not listed component. Phenyl salicylate is another common preservative found in face and hand creams.[9] Prabha et al.[4] observed a patient with positive reaction to phenyl salicylate using more than five face creams. In our study, four patients tested positive to phenyl salicylate and were using more than three fairness creams. Butyl hydrate is an ingredient in ponds cream which was tested positive in two patients with relevance in one of them. Cetrimide, an antiseptic and major formulation excipient chemical in cosmetics, is reported to elicit positive reactions in 12% of 50 patients with cosmetic dermatitis.[10] In our study, cetrimide was tested positive in three patients (4th common allergen) among those using fairness creams. Hexamine is a solvent in cosmetics and was tested positive in two patients using “Fair and Lovely” fairness and “Vicco turmeric” creams. Patient 3 who was using “Fair and Lovely” cream and Patanjali face wash tested positive to multiple allergens [Table 1]. Among them, cetyl alcohol and sorbic acid are one of the ingredients of “Fair and Lovely” cream. This patient, however, did not test positive with the creams as such. This can be explained by the fact that the ingredients are present in lower concentrations in finished products.
Cosmetic contact sensitivity may be an important cause of melasma. Positive patch test in such cases could be coincidental, but high relevance noted in our study warrants a reconsideration. Manufacturers do not list most of the ingredients in a cosmetic product, so relevance of positive reactions may not possibly be ascertained in all cases. Avoidance of cosmetic contact hypersensitivity could be an essential step in preventing/treating melasma.
Limitations
Small sample size and limited number of cosmetic products were only patch tested.
CONCLUSION
Cosmetic contact sensitivity may be an important cause of melasma. Thiomersal in cosmetic products may be an important allergen to cause melasma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Melasma: An up-to-date comprehensive review. Dermatol Ther (Heidelb). 2017;7:305-18.
- [CrossRef] [PubMed] [Google Scholar]
- Pigmented cosmetic dermatitis. Int J Dermatol. 1984;23:299-305.
- [CrossRef] [PubMed] [Google Scholar]
- Cosmetic contact sensitivity in patients with melasma: Results of a pilot study. Dermatol Res Pract. 2014;2014:316219.
- [CrossRef] [PubMed] [Google Scholar]
- Melasma: Etiologic and therapeutic considerations. Arch Dermatol. 1995;131:1453-7.
- [CrossRef] [PubMed] [Google Scholar]
- Does low mercury containing skin-lightening cream (fair and lovely) affect the kidney, liver, and brain of female mice? Cutan Ocul Toxicol. 2005;24:11-29.
- [CrossRef] [PubMed] [Google Scholar]
- Contact allergies to cosmetics: Testing with 52 cosmetic ingredients and personal products. J Dermatol. 2005;32:951-5.
- [CrossRef] [PubMed] [Google Scholar]
- Allergy to phenyl salicylate. Contact Dermatitis. 1981;7:208-11.
- [CrossRef] [PubMed] [Google Scholar]




