
Translate this page into:
Dermoscopy of molluscum contagiosum with an orifice-single lesion in an adult


*Corresponding author: Vishal Gaurav, Department of Dermatology and Venereology, Maulana Azad Medical College, New Delhi, India. mevishalgaurav@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gaurav V, Bahadur A. Dermoscopy of molluscum contagiosum with an orifice-single lesion in an adult. CosmoDerma. 2024;4:91. doi: 10.25259/CSDM_87_2024
Dear Sir,
Molluscum contagiosum (MC) is a common viral infection of the skin that often presents as small dome-shaped papules with central umbilication.[1] While typically straightforward to diagnose, MC can occasionally present as solitary or inflamed lesions, complicating the clinical picture. Dermoscopy enhances the visualization of characteristic features of MC, such as central white structures and specific vascular patterns, aiding in differential diagnosis from other umbilicated lesions such as sebaceous hyperplasia, keratoacanthoma, and basal cell carcinoma (BCC). This report details the case of a 55-year-old female with a solitary papule on the forehead, emphasizing the role of dermoscopy in confirming the diagnosis and guiding effective treatment.
A 55-year-old female presented with an asymptomatic solitary papule on the left side of her forehead for two months. The patient had no significant medical history or immunosuppressive conditions. On examination, a discrete, dome-shaped, flesh-colored papule with central umbilication, measuring 3 mm in diameter was noted on the left side of the forehead [Figure 1]. Dermoscopy was done with a clinical diagnosis of MC to rule out sebaceous hyperplasia, keratoacanthoma, and BCC. Dermoscopy in polarized mode showed central white structures of variable sizes in a polylobular pattern and mixed vascular pattern consisting of crown and radial vessels [Figure 2]. These dermoscopic features supported the clinical diagnosis of MC. Based on clinical and dermoscopic findings, a diagnosis of MC was made. The patient was informed about the benign nature of the condition. Considering the cosmetic concern due to the facial location, the patient opted for treatment. Curettage was performed under local anesthesia, which expressed cheesy white material. Tzanck smear of expressed material showed ovoid, deeply basophilic virus-transformed keratinocytes with a homogeneous, hyaline structure surrounded by a membrane along with anucleated and degenerated keratinocytes [Figure 3]. Post-procedural care included the application of a topical antibiotic ointment to prevent secondary infection. Follow-up at four weeks showed complete resolution of the lesions with no scarring or recurrence.

- A discrete, dome-shaped, and flesh-colored papule with central umbilication, measuring 3 mm in diameter on the left side of the forehead.

- Polarized dermoscopy (Heine DELTAone) showing central white structures of variable sizes in a polylobular pattern and mixed vascular pattern consisting of crown and radial vessels (×10).
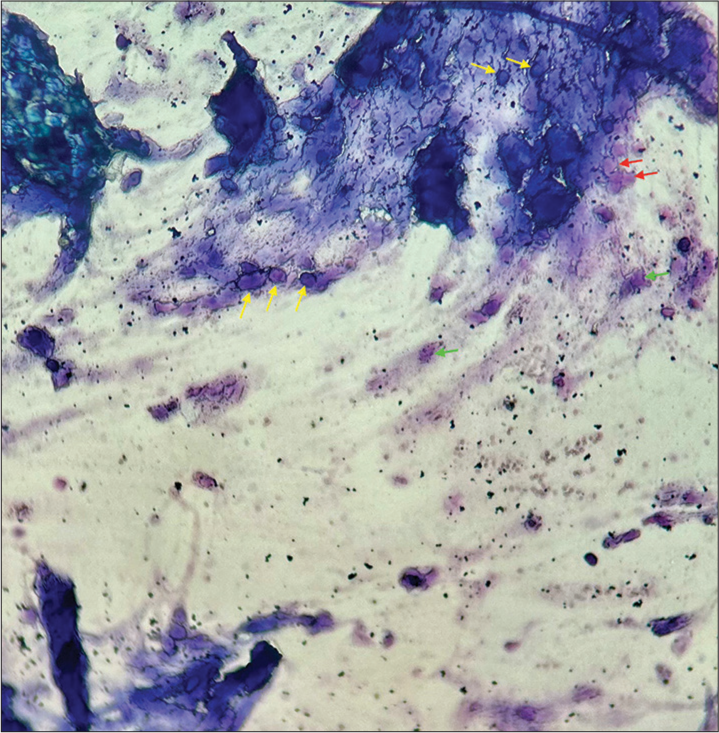
- Tzanck smear of expressed material showing ovoid, deeply basophilic virus-transformed keratinocytes with a homogeneous, hyaline structure surrounded by a membrane along (yellow arrows) with anucleated (red arrows) and degenerated keratinocytes (green arrows) at ×100 magnification.
The dermoscopic patterns of MC are divided into white structures, and vascular patterns (single vascular patterns, and mixed vascular patterns). The white structures include roundish (a solitary whitish area in the center), polylobular (white lesions of variable sizes), and four-leaved clover-like/rosette (white structures in a clover leaf shape) structures. Single vascular patterns consist of radial (vessels perpendicular to the center), crown (vessels encircling the lesion), and punctiform (vessels in a punctate pattern). Mixed vascular patterns are combinations of these features, such as crown with radial, crown with punctiform, and crown with both radial and punctiform patterns.[2] Rosettes have also been described as dermoscopic findings in MC. These are dermoscopic structures characterized by four white points arranged like a four-leaf clover, typically seen over follicular openings under polarized dermoscopy. Initially thought to be specific to actinic keratosis and squamous cell carcinoma, they are now known to appear in various conditions and are considered non-specific. Their exact etiology is unclear, but they are classified with shiny white structures, including shiny white lines and areas associated with fibrosis. The formation of rosettes may result from the interaction of polarized light with narrowed or keratin-filled adnexal openings, or from alternating focal hyperkeratosis and normal stratum corneum. It is believed that rosettes are an optical effect of crossed polarization by concentric fibrosis or horny material, seen frequently over actinic skin. Smaller rosettes (0.1–0.2 mm) arise from the polarization of concentric horn material in follicular and eccrine ducts, while larger rosettes (0.3–0.5 mm) are due to concentric fibrosis around follicles.[3] Ianhez et al., investigated the role of dermoscopy in the diagnosis of MC.[4] Histopathologically confirmed lesions in 57 patients were examined both clinically and dermoscopically. The study evaluated 211 lesions, revealing that orifices were visible in 50.24% of lesions through clinical examination and in 96.68% through dermoscopy. Vascular patterns were identified in 6.16% of lesions clinically and in 89.10% dermoscopically. Among the 188 lesions with visible vessels on dermoscopy, the vascular patterns observed included crown (72.34%), radial (54.25%), and punctiform (20.21%), with half of these lesions exhibiting mixed vascular patterns. Dermoscopy detected more orifices and vessels compared to clinical examination, even in inflamed lesions or those with perilesional eczema. Punctiform vessels were particularly associated with inflammation and excoriation. The white structures correspond histologically to enlarged keratinocytes containing intracytoplasmic viral inclusions and the vascular patterns corresponding to dilated dermal vessels.[4]
Sebaceous hyperplasia, keratoacanthoma, and BCC may also present as umbilicated lesions in this age group. The dermoscopic findings of sebaceous hyperplasia typically include a white-yellowish lobulated structure corresponding to hyperplastic sebaceous gland lobules, umbilication corresponding to the dilated sebaceous gland duct and the follicular orifice, and vascular patterns corresponding to dilated dermal vessels. These vascular patterns often present as crown vessels, irregular vessels, or arborizing vessels.[5] Dermoscopy of keratoacanthoma reveals central yellowish-whitish scaling which corresponds to compact orthokeratotic hyperkeratosis. White circles, indicative of acanthosis and hypergranulosis of the infundibular epithelium, suggest follicular invasion and have the highest specificity. Whitish structures within these circles represent a dilated follicular infundibulum with a keratin plug. In addition, whitish lines and structureless areas correlate with keratinizing tumor cell masses, while red globules within white areas indicate microhemorrhage, or blood spots, within the keratin.[6] The dermoscopic findings in BCC include blue ovoid nests and blue globules corresponding to basaloid tumor islands, leaf-like structures and spoke wheel areas corresponding to stromal retraction, gray-dot granules corresponding to inflammatory cells, arborizing blood vessels corresponding to dilated dermal vessels, porcelain white areas corresponding to thickened collagen fibers, and signs of erosion or ulceration due to loss of the epidermis.[5]
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- "Molluscum" conditions in dermatology. Indian Dermatol Online J. 2021;12:962-5.
- [CrossRef] [PubMed] [Google Scholar]
- Molluscum contagiosum en plaque-an unusual presentation with dermoscopy to rescue. Indian Dermatol Online J. 2023;15:509-11.
- [CrossRef] [PubMed] [Google Scholar]
- Rosette: An additional in vivo dermoscopic finding in molluscum contagiosum. Indian J Paediatr Dermatol. 2019;20:349-50.
- [CrossRef] [Google Scholar]
- Dermoscopic patterns of molluscum contagiosum: A study of 211 lesions confirmed by histopathology. An Bras Dermatol. 2011;86:74-9.
- [CrossRef] [PubMed] [Google Scholar]
- Detection of sebaceous gland hyperplasia with dermoscopy and reflectance confocal microscopy. Front Med (Lausanne). 2023;10:1194748.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatoscopy of solitary keratoacanthoma. Indian J Dermatol. 2022;67:628.
- [CrossRef] [PubMed] [Google Scholar]




