
Translate this page into:
A rare case of blistering distal dactylitis in an adult

*Corresponding author: Shini Choubey, Department of Dermatology, Kalinga Institute of Medical Sciences, Bhubaneshwar, Odisha, India. choubeyshini@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Choubey S, Vinayak K, Begum F. A rare case of blistering distal dactylitis in an adult. CosmoDerma. 2024;4:105. doi: 10.25259/CSDM_120_2024
Dear Sir,
A 62-year-old male patient presented to the out-patient department with multiple painful lesions and swelling of fingers of bilateral hands and bilateral great toe. On further inquiry, the patient was a known case of pelvic tumor, since 2021. He was operated for the same, two years ago with the tissue section histopathology suggestive of a solitary fibrous tumor. Since then, the patient has been in remission. In December 2023, there was a suspicion of relapse and the patient was started with tyrosinase kinase inhibitor pazopanib with a 400 mg once daily dose. Four weeks after starting pazopanib, he started developing pain and redness on the skin overlying the right proximal interphalangeal joint of all fingers and left great toe which, then, progressed to involve both hands and foot along with the development of pus-filled tense bulla over the course of next one week.
On examination, yellowish-white, desquamating lesions along with tender and tense bullae were present involving the palmar and plantar regions, which were consistent with blistering distal dactylitis (BDD)[1] [Figure 1]. The patient was, then, advised for pus culture which showed Methicillin-sensitive Staphylococcus aureus growth and the patient was started on oral antibiotics (Cefixime 200 mg twice daily and clobetasol ointment once daily application) for a week and a diagnosis of BDD was made. The patient was advised to discontinue pazopanib. The patient was reviewed after seven days and the skin lesions had resolved [Figure 2].

- Multiple yellowish-white, tender, and tense bullae present over the palmoplantar region.
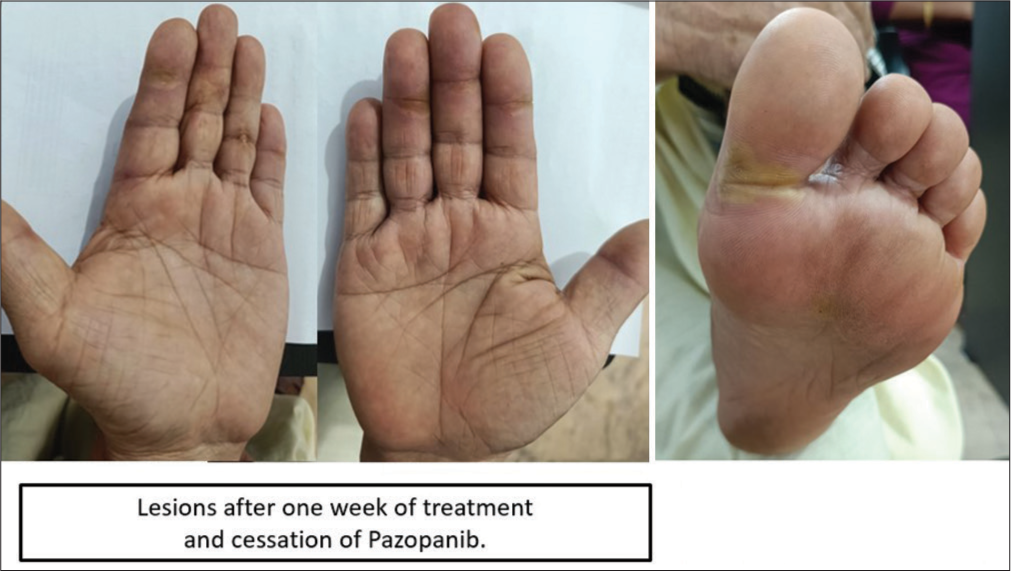
- Lesions subsided after 1 week of supportive therapy and cessation of the drug.
Hays and Mullard initially identified BDD in 1972.[2] It is an uncommon bacterial infection of the finger’s distal phalanx. The causal microbe is generally group A beta-hemolytic Streptococcus, with S. aureus appearing occasionally. It is more frequent in children and adolescents.[3] The BBD is rarely reported in adults, seen in the elderly, diabetic or immunocompromised conditions.[4] Methicillin-resistant S. aureus is relatively infrequently reported worldwide.[5]
In conclusion, it is important to acknowledge this rare entity in adults, which can often be misdiagnosed as to include irritant and allergic contact dermatitis, pompholyx, post-traumatic blisters, blisters caused by thermal injuries, herpetic whitlow, bullous impetigo, erythema multiforme, and epidermolysis bullosa. Even though BDD is never life-threatening, it can have significant detrimental effects on quality of life and cause severe discomfort and functional impairment, particularly in older people. The treatment includes topical and/or systemic antibiotics that are used in addition to incision and drainage if required. No treatment failures have been documented.[6]
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Seven cases of blistering dactylitis. Acta Derm Venereol. 2020;100:5757.
- [CrossRef] [PubMed] [Google Scholar]
- Can nasal bacterial flora be predicted from clinical findings? Pediatrics. 1972;49:596-9.
- [CrossRef] [PubMed] [Google Scholar]
- Blistering distal dactylitis in an adult. J Am Acad Dermatol. 2015;19:397-9.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent blistering distal dactylitis due to Staphylococcus aureus in an immunocompetent elderly woman. BMJ Case Rep. 2018;2018:bcr2017222772.
- [CrossRef] [PubMed] [Google Scholar]
- MRSA blistering distal dactylitis and review of reported cases. Pediatr Dermatol. 2011;28:433-5.
- [CrossRef] [PubMed] [Google Scholar]
- Is blistering distal dactylitis a variant of bullous impetigo? Clin Exp Dermatol. 2007;32:314-6.
- [CrossRef] [PubMed] [Google Scholar]




