
Translate this page into:
Verrucous plaque over lip


*Corresponding author: Tarun Narang, Department of Dermatology, Venereology, and Leprology, PGIMER, Chandigarh, India. priyansh.gupta2412@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta P, Thakur V, Kumar S, Narang T, Chatterjee D. Verrucous plaque over the lip. CosmoDerma. 2024;4:52. doi: 10.25259/CSDM_45_2024
An elderly male farmer presented to our outpatient department with complaints of thick whitish growth over the right side of lower and upper lips for the past five years with a similar whitish plaque on the left side without any associated pain or burning sensation. There was no history of involvement of any other body site. He has been a chronic smoker for the past 20 years. There was no joint pain or significant drug history. Physical examination revealed poorly defined whitish plaque on the right side of the upper and lower lip extending marginally into the right buccal mucosa and crossing the vermillion border on the cutaneous side. The plaque was associated with overlying verrucous growth without any scaling, bleeding or other secondary changes [Figure 1]. In addition, another small similar whitish plaque around 1 × 2 cm was present over the left corner of both lips. No other positive findings were noted on rest of the cutaneous and systemic examination. The lesion of the patient was biopsied for histopathological examination in which the epidermis showed diffuse hyperkeratosis, acanthosis, papillomatosis, basal layer vacuolization, mild pigment incontinence, band-like infiltrate at the dermoepidermal junction, and a moderate degree of chronic inflammatory infiltrate in the upper dermis and perivascular areas [Figures 2a and b]. No evidence of hypergranulosis, apoptotic keratinocytes, dysplastic changes or any invasion was seen. The anti-nuclear antibody of the patient was strongly positive 2+, homogenous pattern, but his hematological and biochemical investigations, urine examination, and chest x-ray were normal. Complement levels were normal, and the anti-phospholipid antibody profile was normal.

- Clinical image of the lip showing ill-defined verrucous plaque over the right upper and lower lip extending to the buccal mucosa and crossing vermillion border on cutaneous side.
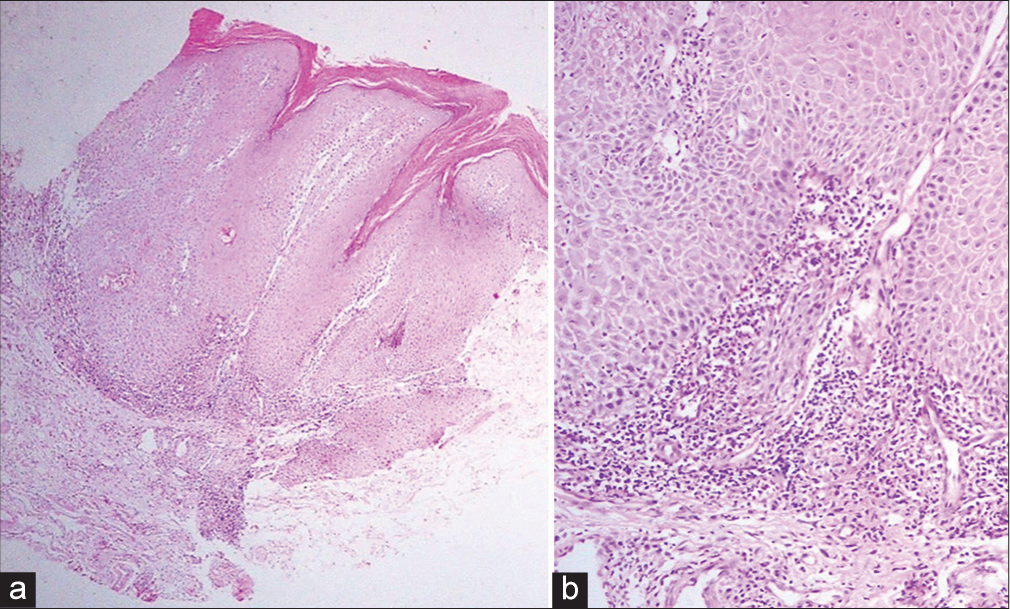
- (a) Histopathological image of the plaque on the right side showing shows verrucous hyperplasia of the epidermis and a band-like infiltrate at the dermoepidermal junction (hematoxylin and eosin ×40). (b) Higher magnification of the histopathological image of dermoepidermal junction showing basal layer vacuolization, mild pigment incontinence, and a moderate degree of chronic inflammatory infiltrate in the upper dermis (hematoxylin and eosin ×200).
WHAT IS YOUR DIAGNOSIS?
Answer:
Verrucous discoid lupus erythematosus (DLE).
DISCUSSION
Cutaneous manifestations of systemic lupus erythematosus can be divided into acute, subacute, and chronic lupus erythematosus lesions on the basis of clinical presentation and disease courses. The DLE, a type of chronic cutaneous lupus erythematosus, has various morphological variants with rare forms including verrucosus, gyratus repens, comedonicus, and lupus erythematosus telangiectoides. Verrucous DLE is a relatively rare variant with soles as the most commonly affected site. Verrucous/hypertrophic DLE consists of approximately 2% of cutaneous lupus erythematosus.[1] Mucosal hypertrophic DLE lesions occurring in the absence of cutaneous lesions, as seen in this patient, are rare. Hyperkeratotic plaques can also mimic squamous cell carcinoma (SCC) and hypertrophic lichen planus. Other morphologies of verrucous DLE include disseminated papulonodular verrucous lesions, hypertrophic ulcers, and hyperkeratotic plaques on the extremities.[1] Verrucous DLE follows the chronic and refractory course. Mucosal lesions are more refractory to treatment than cutaneous lesions.[2] The other clinical differentials considered in our case include hypertrophic lichen planus and SCC. The absence of other cutaneous manifestations of lichen planus, no hypergranulosis, and lymphocyte poor interface dermatitis on histopathology and positive antinuclear antibody status favored verrucous DLE over lichen planus. The patient was started on acitretin (25 mg/day) and is currently under follow-up. Histopathology is necessary to rule out SCC or features of dysplasia, and it is prudent to biopsy the patient in all such cases. Management options include hydroxychloroquine, intralesional triamcinolone, acitretin, isotretinoin, and thalidomide.[3] Patients should be regularly followed up both clinically and histologically to look for the development of SCC in long-standing lesions.
CONCLUSION
Our case presented a rare variant of DLE at a rare site, verrucous DLE of the mucosa. Knowledge of these lesions is important, as they can be easily confused with SCC and hypertrophic lichen planus. In addition, lesions of verrucous DLE are themselves at risk for progression to SCC. Thus, histopathology with high clinical suspicion is essential to exclude possible malignancy developing in the plaque.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Extensive hypertrophic lupus erythematosus: Atypical presentation. Indian J Dermatol. 2012;57:504.
- [CrossRef] [Google Scholar]
- Hypertrophic (verrucous) cutaneous lupus erythematosus of the lip and oral cavity: A series of 4 cases. Acta Derm Venereol. 2013;93:108-9.
- [CrossRef] [PubMed] [Google Scholar]
- A rare presentation of verrucous/hypertrophic lupus erythematosus: A variant of cutaneous LE. Indian Dermatol Online J. 2014;5:87-8.
- [CrossRef] [PubMed] [Google Scholar]




